The Surgical Outcome of Unstable Distal Clavicle Fractures Treated with 2.4 mm Volar Distal Radius Locking Plate
- Affiliations
-
- 1Department of Orthopedic Surgery, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. osd11@paik.ac.kr
- KMID: 1774095
- DOI: http://doi.org/10.12671/jkfs.2015.28.1.38
Abstract
- PURPOSE
This study evaluated the surgical outcomes of unstable distal clavicular fractures treated with a 2.4 mm volar distal radius locking plate.
MATERIALS AND METHODS
From August 2009 to August 2012, 16 patients with distal clavicle fractures underwent surgical treatment. Mean age was 36 years (18-62 years) and mean follow-up period was 12.9 months (6-32 months). Two cases were Neer type I, six cases IIa, three cases IIb, three cases III, and two cases V. For the radiologic assessment, union time and metal failure were evaluated, and coracoidiologic assessment, union time and metal failure were evaluatethe acromioclavicular joint. The clinical results were evaluated by range of motion, postoperative complication, and University of California at Los Angeles (UCLA) score.
RESULTS
Mean time to fracture union was 7.4 weeks (6-14 weeks) in all cases. No statistical difference in coracoid-clavicle distance was observed between immediate post-operation group and contra-lateral group (p=0.6), but an increase of 2.1 mm was observed in the last follow up group compared with the contra-lateral group (p<0.01). The UCLA scoring system showed excellent results in 15 cases and good results in one case. Acromial-clavicle instability occurred in one case so that metal removal and distal clavicle resection were performed.
CONCLUSION
A 2.4 mm volar distal radius locking plate can provide rigid fixation through several screw fixation in the short distal fragment and lead to satisfactory clinical outcomes in unstable distal clavicular fractures.
MeSH Terms
Figure
-
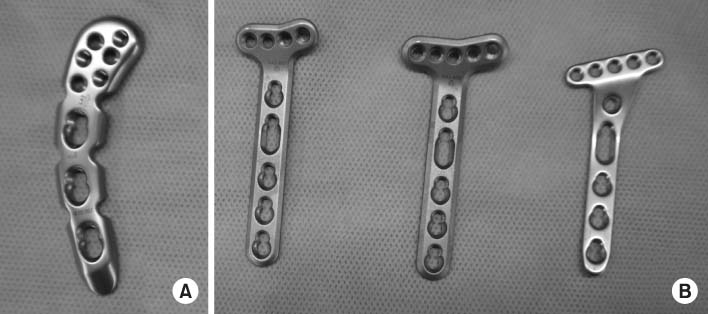
Fig. 1 (A) Precontoured locking plate for distal clavicle (3.5 mm LCP superior clavicle plates; Synthes, Oberdorf, Switzerland). (B) A 2.4 mm volar distal locking plate (2.4 mm LCP Distal Radius System; Synthes) can provide variable options for screw position at the distal clavicle end compared to conventional precontoured locking plate for distal clavicle.
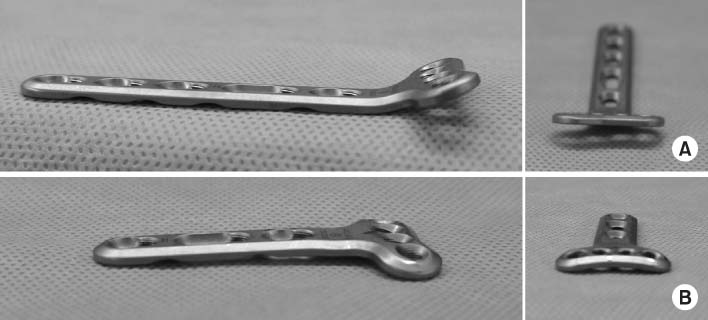
Fig. 2 (A) Original shape of 2.4 mm volar distal radius locking plate. (B) After neutralization of volar angle and making a curved shape from the straight distal end of 2.4 mm volar distal radius locking plate.
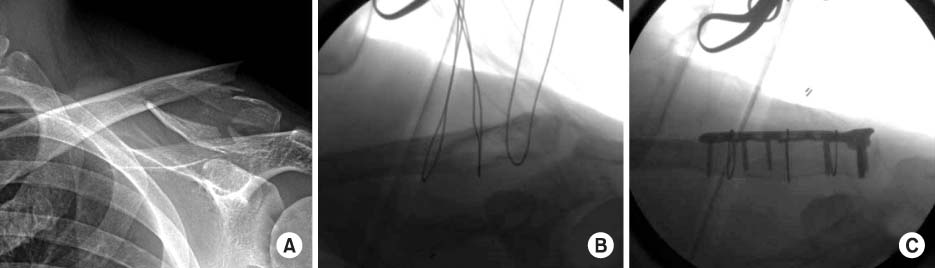
Fig. 3 (A) Preoperative clavicle anteroposterior view of a 41-year-old male shows a Neer V unstable distal clavicle fracture. (B) Intraoperative fluoroscopic image. Cerclage wires were used to stabilize the inferior fragment of the distal clavicle, which is the insertion site of the coraco-clavicular ligament. (C) Intraoperative fluoroscopic image. Short distal fragment could be stabilized by 2.4 volar locking plate for distal radius.
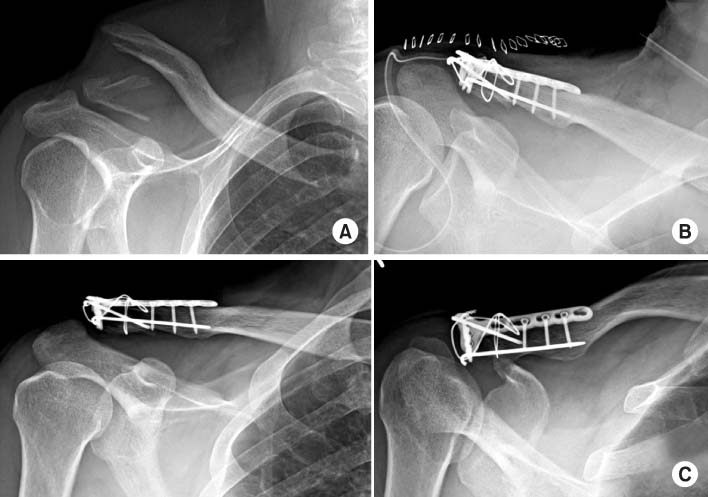
Fig. 4 (A) Preoperative clavicle anteroposterior (AP) view of a 46-year-old male shows a Neer V unstable distal clavicle fracture. (B) Immediate postoperative clavicle AP view of tension band wiring addition to plate fixation. (C) Postoperative four months clavicle AP and apical view shows solid union of the fracture site.
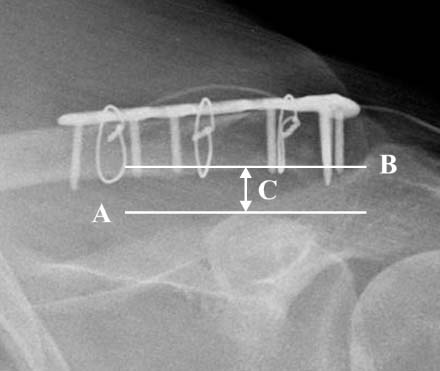
Fig. 5 Measurement of Coracoid-clavicle distance. Coracoidclavicle distance (C) was measured by two parallel lines at the inferior border of the distal clavicle (B) and superior margin of the coracoid process (A).

Fig. 6 (A) Preoperative radiograph of a 42-year-old male shows a Near V unstable distal clavicle fracture. (B) At postoperative 5 months, acromio-clavicle joint dislocation developed as a complication. (C) Removal of plate and distal clavicle resection was performed as a salvage operation.
Reference
-
1. Edwards DJ, Kavanagh TG, Flannery MC. Fractures of the distal clavicle: a case for fixation. Injury. 1992; 23:44–46.
Article2. Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta Orthop Scand. 1993; 64:87–91.
Article3. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am. 2004; 86:778–782.
Article4. Eskola A, Vainionpää S, Pätiälä H, Rokkanen P. Outcome of operative treatment in fresh lateral clavicular fracture. Ann Chir Gynaecol. 1987; 76:167–169.5. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res. 1968; 58:43–50.6. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand. 2002; 73:50–53.
Article7. Kalamaras M, Cutbush K, Robinson M. A method for internal fixation of unstable distal clavicle fractures: early observations using a new technique. J Shoulder Elbow Surg. 2008; 17:60–62.
Article8. Page RS, Bhatia DN. Noncomminuted lateral end clavicle fractures associated with coracoclavicular ligament disruption: Technical considerations for optimal anatomic fixation and stability. Int J Shoulder Surg. 2014; 8:86–89.
Article9. Nuber GW, Bowen MK. Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg. 1997; 5:11–18.
Article10. Kao FC, Chao EK, Chen CH, Yu SW, Chen CY, Yen CY. Treatment of distal clavicle fracture using Kirschner wires and tension-band wires. J Trauma. 2001; 51:522–525.
Article11. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987; 214:160–164.
Article12. Hessmann M, Kirchner R, Baumgaertel F, Gehling H, Gotzen L. Treatment of unstable distal clavicular fractures with and without lesions of the acromioclavicular joint. Injury. 1996; 27:47–52.
Article13. Tsai CH, Hsu HC, Huan CY, Chen HT, Fong YC. Late migration of threaded wire (schanz screw) from right distal clavicle to the cervical spine. J Chin Med Assoc. 2009; 72:48–51.
Article14. Ballmer FT, Gerber C. Coracoclavicular screw fixation for unstable fractures of the distal clavicle. A report of five cases. J Bone Joint Surg Br. 1991; 73:291–294.
Article15. Goldberg JA, Bruce WJ, Sonnabend DH, Walsh WR. Type 2 fractures of the distal clavicle: a new surgical technique. J Shoulder Elbow Surg. 1997; 6:380–382.
Article16. Charity RM, Haidar SG, Ghosh S, Tillu AB. Fixation failure of the clavicular hook plate: a report of three cases. J Orthop Surg (Hong Kong). 2006; 14:333–335.
Article17. Sim E, Schwarz N, Höcker K, Berzlanovich A. Repair of complete acromioclavicular separations using the acromioclavicular-hook plate. Clin Orthop Relat Res. 1995; 314:134–142.
Article18. Faraj AA, Ketzer B. The use of a hook-plate in the management of acromioclavicular injuries. Report of ten cases. Acta Orthop Belg. 2001; 67:448–451.19. Salem KH, Schmelz A. Treatment of Tossy III acromioclavicular joint injuries using hook plates and ligament suture. J Orthop Trauma. 2009; 23:565–569.
Article20. Banerjee R, Waterman B, Padalecki J, Robertson W. Management of distal clavicle fractures. J Am Acad Orthop Surg. 2011; 19:392–401.
Article21. Basamania CJ, Rockwood CA. Fractures of the clavicle. In : Rockwood CA, editor. The shoulder. 4th ed. Philadelphia: WB Saunders;2009. p. 428–482.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Failure of Distal Locking Screws in an Intraarticular Distal Radius Fracture Treated with Volar Locking Plate Fixation
- External Fixation for Distal Radius Fractures
- Short Term Results of Operative Management with 2.4 mm Volar Locking Compression Plates in Distal Radius Fractures
- Volar T-Locking Compression Plate for Treatment of Unstable Distal Radius Fractures
- Relationship between the Length of Distal Locking Screws and Diaphyseal Screws in Volar Plate Fixation of Distal Radius Fractures
