Catheter Ablation of Multiple Accessory Pathways in Duchenne Muscular Dystrophy
- Affiliations
-
- 1Krankenanstalt Rudolfstiftung, Vienna, Austria. fifigs1@yahoo.de
- 2Second Medical Department, Krankenanstalt Rudolfstiftung, Vienna, Austria.
- KMID: 1769647
- DOI: http://doi.org/10.4070/kcj.2013.43.2.115
Abstract
- A 23-year-old male with Duchenne muscular dystrophy (DMD) experienced self-limiting palpitations at age 19 years for the first time. Palpitations recurred not earlier than at age 23 years, and were attributed to narrow complex tachycardia, which could be terminated with adenosine. Since electrocardiography showed a delta-wave, Wolff-Parkinson-White (WPW) syndrome was diagnosed, ajmaline prescribed and radio-frequency catheter ablation of three accessory pathways carried out one week later. One day after ablation, however, a relapse of the supraventricular tachycardia occurred and was terminated with ajmaline. Re-entry tachycardia occurred a second time six days after ablation, and as before, it was stopped only with ajmaline. Despite administration of verapamil to prevent tachycardia, it occurred a third time four months after ablation. This case shows that cardiac involvement in DMD may manifest also as WPW-syndrome. In these patients, repeated radio-frequency catheter ablation of accessory pathways may be necessary to completely block the re-entry mechanism.
MeSH Terms
Figure
-
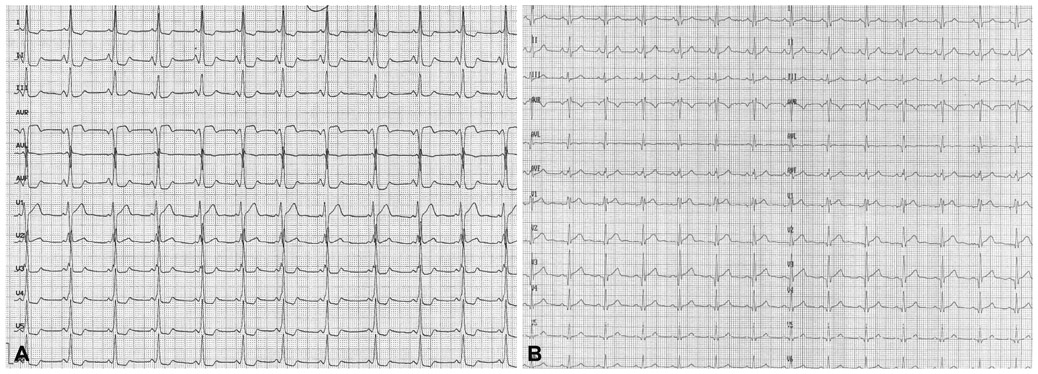
Fig. 1 ECG on admission showing shortening of the PQ-interval and a delta-wave over all chest wall recordings (A). ECG 12 days after the ablation shows incomplete right bundle branch block and small Q-waves over V 2-6, but no longer pre-excitation (B). ECG: electrocardiography.
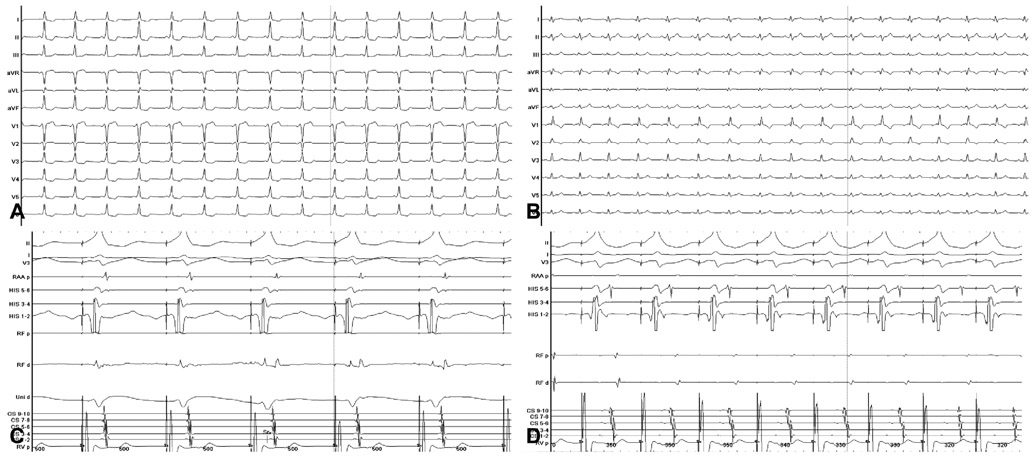
Fig. 2 Surface ECG before ablation with delta-wave (A) and after ablation without delta-wave (B). Intracardiac ECG before ablation (C) and after bump of the accessory pathway (D). The left lower panel shows change of the retrograde activation pattern during energy delivery (3rd beat from the right) with a shift to the second exclusively retrograde conducting right postero-septal accessory pathway. The right lower panel shows the retrograde activation pattern after ablation with exclusive conduction via the retrograde conducting AV-node. ECG: electrocardiography, AV: atrioventricular.
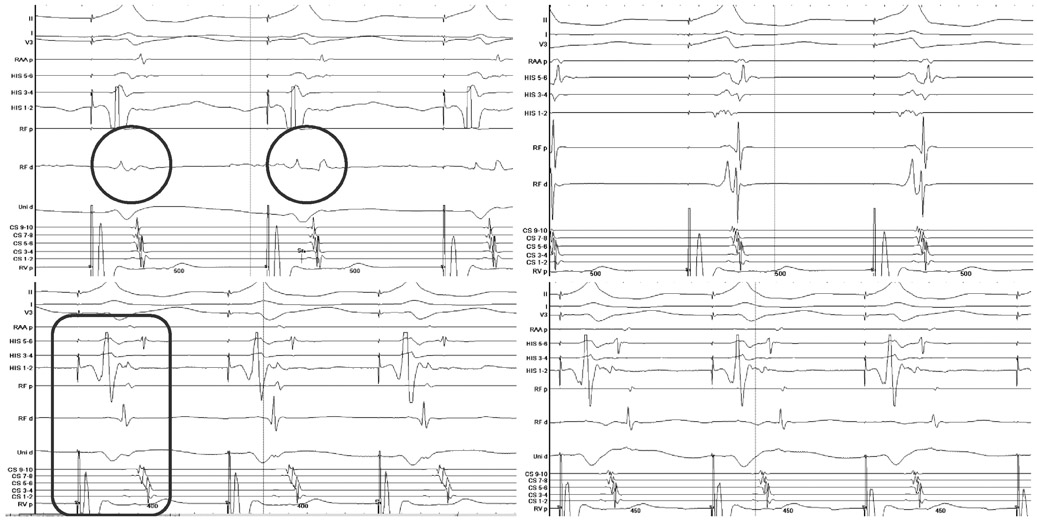
Fig. 3 The left upper panel shows change of the retrograde activation pattern during energy delivery with a shift from the right anterior septal pathway (circle) to the right postero-septal pathway (circle). The right upper panel shows the target signal for the right postero-septal pathway. The right anterolateral accessory pathway with exclusively retrograde conduction (encircled) is shown in the left lower panel. Retrograde conduction via the AV-node after ablation is shown in the right lower panel. The ablation of the antero-lateral pathway was achieved by energy delivery via an Agilis long sheath during sinus rhythm. AV: atrioventricular.
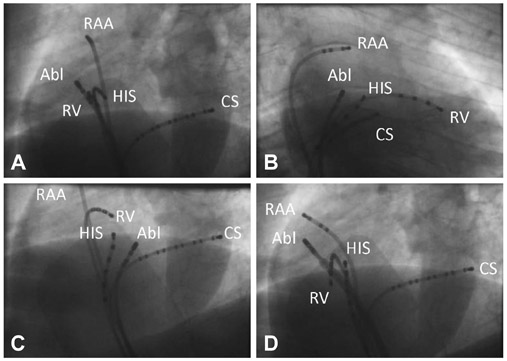
Fig. 4 Catheter position during ablation of the 1. accessory, anterograde and retrograde conducting, right antero-septal pathway in LAO 45° (A) and in RAO 30° (B), of the 2. accessory exclusively retrograde conducting right posterior-septal pathway in LAO 45° (C), and during ablation of the 3. accessory, exclusively retrograde conducting right posterior-lateral pathway in LAO 45° (D). A stable position at the tricuspid anulus was achieved only with the steerable introducer Agilis NxT (St. Jude Medical). RV: right ventricle, HIS: HIS bundle, RAA: right atrial appendage, CS: coronary sinus, Abl: ablation catheter, LAO: left anterior oblique, RAO: right anterior oblique.
Reference
-
1. Finsterer J, Stöllberger C. The heart in human dystrophinopathies. Cardiology. 2003. 99:1–19.2. Agarwal RK, Misra DN, Verma RK. Wolff-Parkinson-White syndrome with paroxysmal atrial fibrillation in pseudohypertrophic muscular dystrophy (Duchenne type). Indian Heart J. 1973. 25:346–348.3. Finsterer J, Stöllberger C, Quasthoff S. Wolff-Parkinson-White syndrome as initial manifestation of Becker muscular dystrophy. Herz. 2008. 33:307–310.4. Symons AL, Townsend GC, Hughes TE. Dental characteristics of patients with Duchenne muscular dystrophy. ASDC J Dent Child. 2002. 69:277–283. 2345. Weiss C, Jakubiczka S, Huebner A, et al. Tandem duplication of DMD exon 18 associated with epilepsy, macroglossia, and endocrinologic abnormalities. Muscle Nerve. 2007. 35:396–401.6. Kirchmann C, Kececioglu D, Korinthenberg R, Dittrich S. Echocardiographic and electrocardiographic findings of cardiomyopathy in Duchenne and Becker-Kiener muscular dystrophies. Pediatr Cardiol. 2005. 26:66–72.7. Sethi KK, Dhall A, Chadha DS, Garg S, Malani SK, Mathew OP. WPW and preexcitation syndromes. J Assoc Physicians India. 2007. 55:Suppl. 10–15.8. Cay S, Topaloglu S, Aras D. Percutenous catheter ablation of the accessory pathway in a patient with wolff-Parkinson-white syndrome associated with familial atrial fibrillation. Indian Pacing Electrophysiol J. 2008. 8:141–145.9. Bodalski R, Maryniak A, Walczak F, Szumowski L, Jedynak Z. [Glass of water or ablation?-episodes of malignant atrial tachyarrhythmias during swimming in a lake in a woman with overt Wolff-Parkinson-White syndrome and benign palpitations for several decades of life]. Kardiol Pol. 2008. 66:1346–1349.10. Tischenko A, Fox DJ, Yee R, et al. When should we recommend catheter ablation for patients with the Wolff-Parkinson-White syndrome? Curr Opin Cardiol. 2008. 23:32–37.11. Ghosh S, Rhee EK, Avari JN, Woodard PK, Rudy Y. Cardiac memory in patients with Wolff-Parkinson-White syndrome: noninvasive imaging of activation and repolarization before and after catheter ablation. Circulation. 2008. 118:907–915.12. Light PE. Familial Wolff-Parkinson-White Syndrome: a disease of glycogen storage or ion channel dysfunction? J Cardiovasc Electrophysiol. 2006. 17:Suppl 1. S158–S161.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A clinical study on Duchenne muscular dystrophy
- Duchenne Muscular Dystrophy Complicated With Dilated Cardiomyopathy and Cerebral Infarction
- A Clinical Study on Duchenne Muscular Dystrophy in Childhood
- Duchenne Type Muscular Dystrophy: Report of 8 Cases
- Carrier detection of duchenne muscular dystrophy with closelylinked RFLPs.
