Visual Prognosis of Retinoblastoma in the Posterior Pole Treated with Primary Chemotherapy Plus Local Treatments
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. ysyu@snu.ac.kr
- 2Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- 3Department of Pediatrics, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1769088
- DOI: http://doi.org/10.3341/kjo.2010.24.6.347
Abstract
- PURPOSE
To evaluate the visual outcomes of retinoblastoma in the posterior pole (RBPP) treated with chemotherapy plus local treatments and to address the prognostic factors that influence such outcomes.
METHODS
The medical records of patients with RBPP diagnosed at the Department of Pediatric Ophthalmology, Seoul National University Children's Hospital between August 1987 and September 2007 were reviewed retrospectively. Only those patients treated via primary chemotherapy plus local treatments were included. The presence of foveal involvement and tumors in the posterior pole before and after treatment, the type of regression pattern and the best corrected visual acuity (BCVA) of each patient were evaluated.
RESULTS
A total of 13 eyes in 12 patients were included. The mean final BCVA for treated RBPP was 20/210 (range, hand motion to 20/16). However, eight eyes (61.5%) had an acuity of 20/200 or better and seven eyes (53.8%) had an acuity of 20/50 or better. The mean final BCVA was significantly better in cases with negative foveal involvement; however, four eyes (37.5%) with positive foveal involvement had an acuity of 20/200 or better. Tumors area in the posterior pole and the type of regression pattern were not significantly related to final BCVA.
CONCLUSIONS
Over one half of the studied RBPP patients had working vision. Although the eyes had RBPP with positive foveal involvement, about one-third of the patients had working vision. Vision preservation should be considered when deciding on RBPP treatment.
Keyword
MeSH Terms
-
Antibiotics, Antineoplastic/administration & dosage
Antineoplastic Agents/administration & dosage
Antineoplastic Agents, Alkylating/administration & dosage
Antineoplastic Combined Chemotherapy Protocols/*therapeutic use
Cisplatin/administration & dosage
Cyclophosphamide/administration & dosage
Doxorubicin/administration & dosage
Etoposide/administration & dosage
Eyeglasses
Female
Follow-Up Studies
Fovea Centralis/pathology
Humans
Infant
Male
Prognosis
Retinal Neoplasms/*drug therapy/pathology/*physiopathology
Retinoblastoma/*drug therapy/pathology/*physiopathology
Retrospective Studies
Treatment Outcome
Visual Acuity
Figure
-

Fig. 1 Representative fundus photographs of retinoblastoma in the posterior pole (RBPP) according to foveal involvement and tumor area. Note that cases with tumors either partially or entirely within the posterior pole at diagnosis were considered as RBPP. (A) A representative fundus photograph of RBPP with positive foveal involvement and a tumor larger than half the size of the posterior pole. (B) A representative fundus photograph of RBPP with positive foveal involvement and a tumor less than half the size of the posterior pole. (C) A representative fundus photograph of RBPP with negative foveal involvement and a tumor less than half of the size of posterior pole.

Fig. 2 Distribution of final best corrected visual acuity (BCVA) according to foveal involvement. Note that the final BCVAs were higher in cases of negative foveal involvement. Group F+ represents positive foveal involvement, and group F- represents negative foveal involvement.
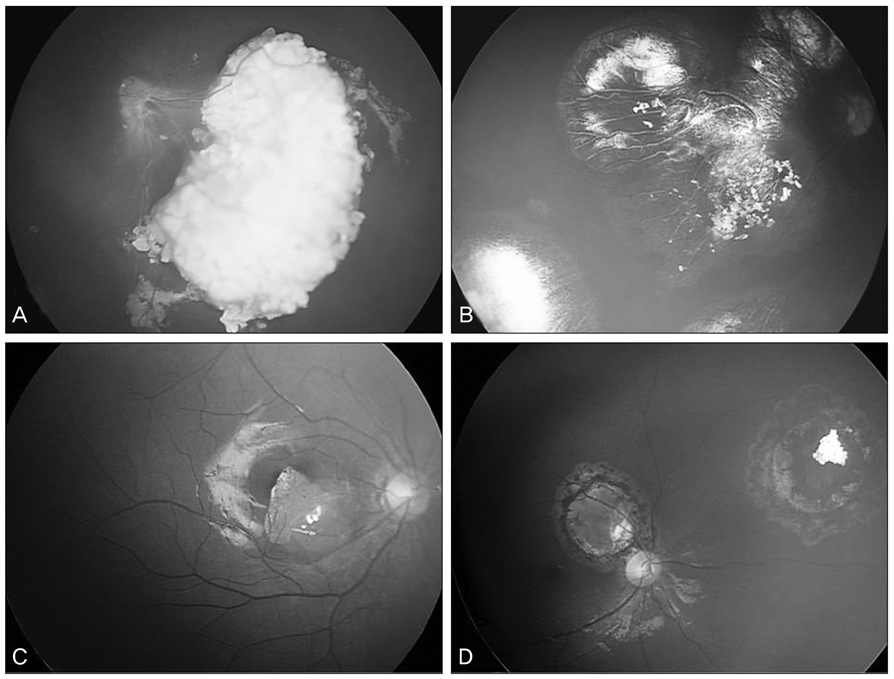
Fig. 3 Representative fundus photographs according to foveal involvement and visual outcome. (A) Eye 4, a representative case of retinoblastoma in the posterior pole (RBPP) with positive foveal involvement, showed a poor visual outcome, with a final best corrected visual acuity (BCVA) of finger counting at 2 feet. (B) Eye 1 had a final BCVA of 20/50. (B,C) Representative cases of RBPP with positive foveal involvement showing fair and good visual outcomes. (C) Eye 8 had a final BCVA of 20/25. (D) A representative case of RBPP with negative foveal involvement showing a good visual outcome; eye 11 had a final BCVA of 20/20.

Fig. 4 Distribution of final best corrected visual acuity (BCVA) according to tumor size. Group L (large) represents tumors greater than half of the size of posterior pole; group S (small) represents tumors less than half of the size of posterior pole. Note that only eyes with foveal involvement were included to avoid the influence of foveal involvement.
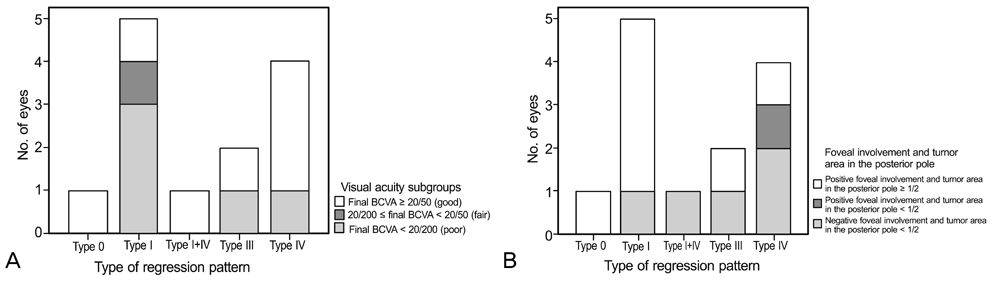
Fig. 5 Distribution of final best corrected visual acuity (BCVA) and status of foveal involvement and tumor area in the posterior pole according to the type of regression pattern. (A) Distribution of final best corrected visual acuity according to the type of regression pattern. Note that the eyes with type IV regression patterns tended to have better final BCVAs than did those of other regression types. (B) The distributions of foveal involvement and tumor size according to the type of the regression pattern. Note that the eyes with type IV regression patterns tended to have less frequent foveal involvements and smaller tumor sizes.
Cited by 1 articles
-
Outcomes of Cataract Surgery Following Treatment for Retinoblastoma
Hyeong Min Kim, Byung Joo Lee, Jeong Hun Kim, Young Suk Yu
Korean J Ophthalmol. 2017;31(1):52-57. doi: 10.3341/kjo.2017.31.1.52.
Reference
-
1. Sanders BM, Draper GJ, Kingston JE. Retinoblastoma in Great Britain 1969-80: incidence, treatment, and survival. Br J Ophthalmol. 1988. 72:576–583.2. Gallie BL, Budning A, DeBoer G, et al. Chemotherapy with focal therapy can cure intraocular retinoblastoma without radiotherapy. Arch Ophthalmol. 1996. 114:1321–1328.3. Murphree AL. Traboulsi EI, editor. Retinoblastoma. Genetic diseases of the eye. 1998. Oxford: Oxford University Press;813–849.4. Murphree AL, Villablanca JG, Deegan WF 3rd, et al. Chemotherapy plus local treatment in the management of intraocular retinoblastoma. Arch Ophthalmol. 1996. 114:1348–1356.5. Abramson DH, Gerardi CM, Ellsworth RM, et al. Radiation regression patterns in treated retinoblastoma: 7 to 21 years later. J Pediatr Ophthalmol Strabismus. 1991. 28:108–112.6. Fontanesi J, Pratt CB, Hustu HO, et al. Use of irradiation for therapy of retinoblastoma in children more than 1 year old: the St. Jude Children's Research Hospital experience and review of literature. Med Pediatr Oncol. 1995. 24:321–326.7. Yu YS, Kim IH, Ahn HS. Late-onset osteosarcoma in bilateral retinoblastoma survivor. J Korean Ophthalmol Soc. 1996. 37:1349–1353.8. Hall LS, Ceisler E, Abramson DH. Visual outcomes in children with bilateral retinoblastoma. J AAPOS. 1999. 3:138–142.9. Lam BL, Judisch GF, Sobol WM, Blodi CF. Visual prognosis in macular retinoblastomas. Am J Ophthalmol. 1990. 110:229–232.10. Migdal C. Bilateral retinoblastoma: the prognosis for vision. Br J Ophthalmol. 1983. 67:592–595.11. Weiss AH, Karr DJ, Kalina RE, et al. Visual outcomes of macular retinoblastoma after external beam radiation therapy. Ophthalmology. 1994. 101:1244–1249.12. Desjardins L, Chefchaouni MC, Lumbroso L, et al. Functional results after treatment of retinoblastoma. J AAPOS. 2002. 6:108–111.13. Schefler AC, Cicciarelli N, Feuer W, et al. Macular retinoblastoma: evaluation of tumor control, local complications, and visual outcomes for eyes treated with chemotherapy and repetitive foveal laser ablation. Ophthalmology. 2007. 114:162–169.14. Singh AD, Garway-Heath D, Love S, et al. Relationship of regression pattern to recurrence in retinoblastoma. Br J Ophthalmol. 1993. 77:12–16.15. Holbek S, Ehlers N. Long-term visual results in eyes cured for retinoblastoma by radiation. Acta Ophthalmol (Copenh). 1989. 67:560–566.16. Buckley EG, Heath H. Visual acuity after successful treatment of large macular retinoblastoma. J Pediatr Ophthalmol Strabismus. 1992. 29:103–106.17. Lueder GT, Goyal R. Visual function after laser hyperthermia and chemotherapy for macular retinoblastoma. Am J Ophthalmol. 1996. 121:582–584.18. Shields CL, Mashayekhi A, Cater J, et al. Chemoreduction for retinoblastoma. Analysis of tumor control and risks for recurrence in 457 tumors. Am J Ophthalmol. 2004. 138:329–337.19. Shields CL, Palamar M, Sharma P, et al. Retinoblastoma regression patterns following chemoreduction and adjuvant therapy in 557 tumors. Arch Ophthalmol. 2009. 127:282–290.20. Watts P, Westall C, Colpa L, et al. Visual results in children treated for macular retinoblastoma. Eye (Lond). 2002. 16:75–80.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Three Cases of Trilateral Retinoblastoma
- Eye-Preserving Therapy in Retinoblastoma: Prolonged Primary Chemotherapy Alone or Combined with Local Therapy
- Treatment and Prognosis of Retinoblastoma: Clinicopathologic Analysis of 101 Cases
- A Case of Osteosarcoma Developed in a Patient of Untreated Bilateral Retinoblastoma
- Outcomes of Cataract Surgery Following Treatment for Retinoblastoma
