J Korean Surg Soc.
2009 Nov;77(5):326-332. 10.4174/jkss.2009.77.5.326.
Clinical Experiences of Management of Bile Duct Injuries during Laparoscopic Cholecystectomy
- Affiliations
-
- 1Department of Surgery, Gyeongsang National University School of Medicine, Jinju, Korea. hongsc@nongae.gnu.ac.kr
- KMID: 1750701
- DOI: http://doi.org/10.4174/jkss.2009.77.5.326
Abstract
- PURPOSE
Laparoscopic cholecystectomy (LC) has become the gold standard of management of gallstone disease. LC is associated with a two-to-four times higher incidence of bile duct injury, which is a rare but more serious complication than open cholecystectomy. We reviewed our experiences with the management of bile duct injury during laparoscopic cholecystectomy.
METHODS
From January 1999 to April 2009, 13 patients with bile duct injuries following LC were managed in our hospital. Patients' charts were retrospectively reviewed to analyze perioperative management.
RESULTS
Among the 13 patients, 7 patients sustained their bile duct injuries at our hospital. Six patients were referred to our hospital to manage their bile duct injuries. Five patients' injuries were identified during LC. According to the Strasberg classification, there are 5 cases of type A, 2 cases of type C, 1 case of type D and 5 cases of type E injuries. Four type A bile duct injuries were treated by direct ductal ligation during LC and 1 type A bile duct injury and 1 type C bile duct injury were managed by non-surgical treatment. Type D and type E injuries were managed by Roux-en-Y hepaticojejunostomy.
CONCLUSION
Bile duct injuries are a rare but serious complications that occur during laparoscopic cholecystectomy. Most minor bile duct injuries are well treatable with non-surgical management, whereas major bile duct injuries require surgical management. The combination of non-surgical management and surgical treatment results in successful outcomes in bile duct injuries.
MeSH Terms
Figure
-
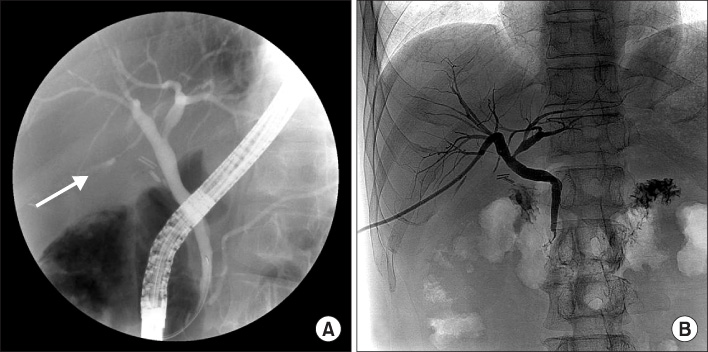
Fig. 1 Type A injury. (A) contrast leakage from the small duct of liver bed is demonstrated (white arrow). (B) 10 days after PTBD, there is no sign of contrast leakage (case 11).
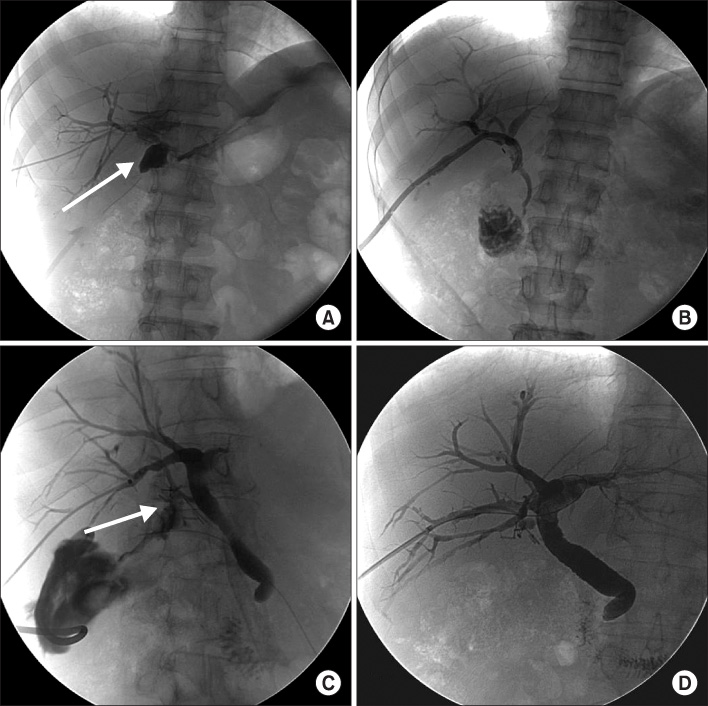
Fig. 2 Type C injury. (A) percutaneous transhepatic cholangiogram shows contrast leakage of right hepatic duct (white arrow, case 4). (B) percutaneous transhepatic cholangiogram performed 3 months later shows no contrast leakage (case 4). (C) contrast leakage from aberrant right hepatic duct is demonstrated (white arrow, case 8). (D) 2 months after, there is no contrast leakage (case 8).
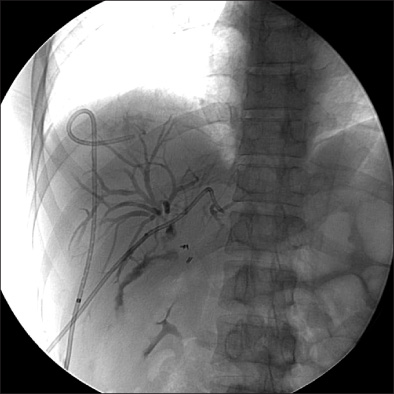
Fig. 3 Percutaneous transhepatic cholangiogram shows type E4 bile duct injury having no communication between right and left hepatic duct (case 12).
Reference
-
1. Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko ST, Airan MC. Complications of laparoscopic cholecystectomy: a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg. 1993. 165:9–14.2. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995. 180:101–125.3. Roslyn JJ, Binns GS, Hughes EF, Saunders-Kirkwood K, Zinner MJ, Cates JA. Open cholecystectomy. A contemporary analysis of 42,474 patients. Ann Surg. 1993. 218:129–137.4. Melton GB, Lillemoe KD, Cameron JL, Sauter PA, Coleman J, Yeo CJ. Major bile duct injuries associated with laparoscopic cholecystectomy: effect of surgical repair on quality of life. Ann Surg. 2002. 235:888–895.5. Boerma D, Rauws EA, Keulemans YC, Bergman JJ, Obertop H, Huibregtse K, et al. Impaired quality of life 5 years after bile duct injury during laparoscopic cholecystectomy: a prospective analysis. Ann Surg. 2001. 234:750–757.6. The Southern Surgeons Club. A prospective analysis of 1518 laparoscopic cholecystectomies. N Engl J Med. 1991. 324:1073–1078.7. Calvete J, Sabater L, Camps B, Verdu A, Gomez-Portilla A, Martin J, et al. Bile duct injury during laparoscopic cholecystectomy: myth or reality of the learning curve? Surg Endosc. 2000. 14:608–611.8. Adamsen S, Hansen OH, Funch-Jensen P, Schulze S, Stage JG, Wara P. Bile duct injury during laparoscopic cholecystectomy: a prospective nationwide series. J Am Coll Surg. 1997. 184:571–578.9. Hugh TB. New strategies to prevent laparoscopic bile duct injury--surgeons can learn from pilots. Surgery. 2002. 132:826–835.10. Debru E, Dawson A, Leibman S, Richardson M, Glen L, Hollinshead J, et al. Does routine intraoperative cholangiography prevent bile duct transection? Surg Endosc. 2005. 19:589–593.11. Ludwig K, Bernhardt J, Steffen H, Lorenz D. Contribution of intraoperative cholangiography to incidence and outcome of common bile duct injuries during laparoscopic cholecystectomy. Surg Endosc. 2002. 16:1098–1104.12. McMahon AJ, Fullarton G, Baxter JN, O'Dwyer PJ. Bile duct injury and bile leakage in laparoscopic cholecystectomy. Br J Surg. 1995. 82:307–313.13. Bergman JJ, van den Brink GR, Rauws EA, de Wit L, Obertop H, Huibregtse K, et al. Treatment of bile duct lesions after laparoscopic cholecystectomy. Gut. 1996. 38:141–147.14. Neuhaus P, Schmidt SC, Hintze RE, Adler A, Veltzke W, Raakow R, et al. Classification and treatment of bile duct injuries after laparoscopic cholecystectomy. Chirurg. 2000. 71:166–173.15. Stewart L, Robinson TN, Lee CM, Liu K, Whang K, Way LW. Right hepatic artery injury associated with laparoscopic bile duct injury: incidence, mechanism, and consequences. J Gastrointest Surg. 2004. 8:523–530.16. Seeliger H, Furst A, Zulke C, Jauch KW. Surgical management of bile duct injuries following laparoscopic cholecystectomy: analysis and follow-up of 28 cases. Langenbecks Arch Surg. 2002. 387:286–293.17. Sikora SS, Kumar A, Das NR, Sarkari A, Saxena R, Kapoor VK. Laparoscopic bile duct injuries: spectrum at a tertiary-care center. J Laparoendosc Adv Surg Tech A. 2001. 11:63–68.18. Keulemans YC, Bergman JJ, de Wit LT, Rauws EA, Huibregtse K, Tytgat GN, et al. Improvement in the management of bile duct injuries? J Am Coll Surg. 1998. 187:246–254.19. Llach J, Bordas JM, Elizalde JI, Enrico C, Gines A, Pellise M, et al. Sphincterotomy in the treatment of biliary leakage. Hepatogastroenterology. 2002. 49:1496–1498.20. Sicklick JK, Camp MS, Lillemoe KD, Melton GB, Yeo CJ, Campbell KA, et al. Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients. Ann Surg. 2005. 241:786–792.21. Melton GB, Lillemoe KD. The current management of postoperative bile duct strictures. Adv Surg. 2002. 36:193–221.22. Stewart L, Way LW. Bile duct injuries during laparoscopic cholecystectomy. Factors that influence the results of treatment. Arch Surg. 1995. 130:1123–1128.23. Schol FP, Go PM, Gouma DJ. Outcome of 49 repairs of bile duct injuries after laparoscopic cholecystectomy. World J Surg. 1995. 19:753–756.24. Kapoor VK. Bile duct injury repair: when? what? who? J Hepatobiliary Pancreat Surg. 2007. 14:476–479.25. Karvonen J, Gullichsen R, Laine S, Salminen P, Gronroos JM. Bile duct injuries during laparoscopic cholecystectomy: primary and long-term results from a single institution. Surg Endosc. 2007. 21:1069–1073.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent classifications of the common bile duct injury
- Laparoscopic cholecystectomy and common bile duct exploration for gallstone and common bile duct stone in a patient with a left-sided gallbladder: a case report
- Intraoperatively malpositioned stent as a complication of common bile duct injury during laparoscopic cholecystectomy
- Endoscopic Management of Bile Leakage after Cholecystectomy: A Single-Center Experience for 12 Years
- Treatments of Proximal Bile Duct Necrosis and Stricture from Iatrogenic Bile Duct Injury of Laparoscopic Cholecystectomy
