J Breast Cancer.
2007 Jun;10(2):169-172. 10.4048/jbc.2007.10.2.169.
Gestational Gigantomastia: A Case Report
- Affiliations
-
- 1Department of Surgery, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. brca@korea.com
- 2Department of Diagnostic Radiology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Obstetrics & Gynecology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 1745065
- DOI: http://doi.org/10.4048/jbc.2007.10.2.169
Abstract
- A 26-yr-old woman (Para: 0-0-0-0) was referred to the breast clinic for the management of bilateral breast enlargement that she experienced at 29 weeks of gestation. The progressive enlargement of both breasts started at 6 weeks of gestation. She also had pain on both her breasts, her shoulders and her back and accompanying skin lesions. On physical examination, the skin over the breasts was red and edematous, with overlying dilated veins. Also on the left side, a patch of desquamation and ulcerative lesion was noticed. Ultrasonography of the breasts showed bilateral parenchymal enlargement with vessel engorgement and ductal dilatation. A 4.2 cm sized well-circumscribed probably benign oval hypoechoic nodule (BI-RADS Category 3) was identified at the upper inner quadrant of the left breast. The patient was conservatively managed until the end of her pregnancy. She delivered a normal full-term baby at 39 weeks of gestation. She did not breast-feed the baby due to severe pain and she revisited the breast clinic at 4 months after the delivery. The size of both breasts was markedly decreased compared to that at the initial visit and the skin lesions on her left breast were completely healed. We report here on the first case of gestational gigantomastia that was treated with conservative care in Korea.
Keyword
MeSH Terms
Figure
-

Fig 1 Pictures of the initial presentation. Both breasts showing massive enlargement. The inferior border reached below the level of umbilicus. The skin over the breasts was red and edematous, with overlying dilated veins. A patch of desquamation and ulcerative lesion was noticed on the left side.
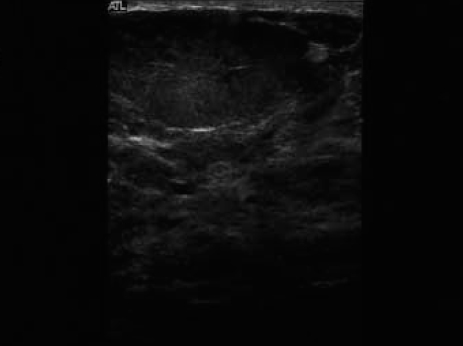
Fig 2 Breast ultrasonographic findings. Ultrasonography of the breasts showed bilateral parenchymal enlargement with vessel engorgement and ductal dilatation. A 4.2 cm sized well-circumscribed probably benign oval hypoechoic nodule (BI-RADS Category 3) was identified at upper inner quadrant of the left breast.
Reference
-
1. Swelstad MR, Swelstad BB, Rao VK, Gutowski KA. Management of gestational gigantomastia. Plast Reconstr Surg. 2006. 118:840–848.
Article2. Agarwal N, Kriplani A, Gupta A, Bhatla N. Management of gigantomastia complicating pregnancy. A case report. J Reprod Med. 2002. 47:871–874.3. Vidaeff AC, Ross PJ, Livingston CK, Parks DH. Gigantomastia complicating mirror syndrome in pregnancy. Obstet Gynecol. 2003. 101:1139–1142.
Article4. Jido TA, Mohamed AZ, Alhasan SU. Gigantomastia complicating pregnancy: a case report. Niger J Med. 2006. 15:167–169.
Article5. Kulkarni D, Beechey-Newman N, Hamed H, Fentiman IS. Gigantomastia: a problem of local recurrence. Breast. 2006. 15:100–102.
Article6. Cha JH, Kim HH, Kim SM, Seo MH, Yoon HS. Breast gigantism induced by D-penicillamine: case report. J Korean Radiol Soc. 2004. 50:213–215.
Article7. Lee JE, Shin HJ, Hwang SE, Hwang KT, Oh SK, Youn YK, et al. A case of breast gigantism in a patient with Wilson's disease treated by penicillamine. J Breast Cancer. 2006. 9:69–72.
Article8. Kaviani A, Hashemi E, Fathi M, Rabbani A. Pregnancy-induced gigantomastia in a 19-year-old woman. Breast J. 2006. 12:495–496.
Article9. Pasrija S, Sharma N. Benign diffuse breast hyperplasia during pregnancy. N Engl J Med. 2006. 355:2771.
Article10. Simpson BS. Notes on a case of diffuse hypertrophy of the breasts. Edinburgh Med J. 1920. 24:176.11. Lewison EF, Jones GS, Trimble FH, da Lima LC. Gigantomastia complicating pregnancy. Surg Gynecol Obstet. 1960. 110:215–223.
Article12. Windom KW, McDuffie RS Jr. Non-Hodgkin's lymphoma presenting with gigantomastia in pregnancy. Obstet Gynecol. 1999. 93:852.
Article13. Gargan TJ, Goldwyn RM. Gigantomastia complicating pregnancy. Plast Reconstr Surg. 1987. 80:121–124.
Article14. Iglehart J, Kaelin C. Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Diseases of the breast. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 2001. 16th ed. Philadelphia: Saunders;555–590.15. Antevski BM, Smilevski DA, Stojovski MZ, Filipovski VA, Banev SG. Extreme gigantomastia in pregnancy: case report and review of literature. Arch Gynecol Obstet. 2007. 275:149–153.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An idiopathic gigantomastia
- Bilateral gigantomastia due to benign breast tumors: a case series and brief review focusing on bilateral diffuse pseudoangiomatous stromal hyperplasia
- Pseudoangiomatous Stromal Hyperplasia of the Breast in a Female Adolescent Presenting as Bilateral Gigantomastia
- Relapsed Bilateral Gigantomastia Caused by Pseudoangiomatous Stromal Hyperplasia after Reduction Mammoplasty
- Primary Ovarian Non-gestational Choriocarcinoma in a Young Women A Case Report
