MR-based Parameters as a Supplement to Radiographs in Managing Developmental Hip Dysplasia
- Affiliations
-
- 1Department of Orthopaedic Surgery, Medical Research Institute, Pusan National University Hospital, Busan, Korea. kimht@pusan.ac.kr
- KMID: 1743910
- DOI: http://doi.org/10.4055/cios.2011.3.3.202
Abstract
- BACKGROUND
Some dysplastic hips with favorable radiographic parameters fail to develop normally, suggesting that we should consider cartilaginous or soft tissue structures for further information regarding the condition of the hip. The purpose of this study was to provide a clear definition of concentric reduction in developmental dysplasia of the hip (DDH) based on magnetic resonance imaging (MRI), and to determine how radiographic and MR-based parameters could be used together to treat dysplastic hips.
METHODS
We studied range of motion (ROM)-MRI of 25 patients with unilateral hip dysplasia (mean age at the time of MR imaging, 44.1 months). Each ROM-MRI consisted of a set of bilateral hip scans in the following positions: neutral; abduction; abduction- internal rotation; abduction-internal rotation-flexion; and adduction. Before MR scanning, the 25 patients received the following primary treatments: closed reduction (n = 15; at a mean age of 14.5 months); and open reduction (n = 10; at a mean age of 10.0 months). The following new parameters appear to be useful in treating DDH: 1) the labral angle, the angle the labrum makes with the acetabulum; 2) the uncorrected labral deformity (ULD), the "residual deformity" (deflection of the labrum) when the affected labrum is freed from pressure in abduction; and 3) the zone of compressive force (ZCF), the region of the acetabulum through which the body weight acts on the femoral head.
RESULTS
A concentrically-reduced hip is one in which the labrum points downward in the neutral position, at the same angle as that of the normal side; and in which the ZCF is zone 3, the inner acetabular zone as defined herein. The ULD and the ZCF may be determined precisely as we have done, or the physician may simply observe the changes in the orientation of the labrum and compare the changes qualitatively to the unaffected side, and likewise for the medial joint space.
CONCLUSIONS
Detailed analysis of the labrum as permitted by ROM-MRI, together with acetabular index and other parameters measured from radiographs, provides important information for physicians treating childhood hip dysplasia.
Keyword
MeSH Terms
Figure
-

Fig. 1 Measurement of labral angle (LA). LA is defined as the angle that the labrum makes with the acetabulum (that is, with the line that is used for measurement of acetabular index [AI]). Line A is the midline of the labrum: that is, it passes through a point midway between the outer and inner attachment points of the labrum (points B and C) and the distal apex of the labrum. Line H is Hilgenreiner's line. The figure shows a dysplastic hip in neutral; such hips have LA values that are high in neutral and low in abduction.
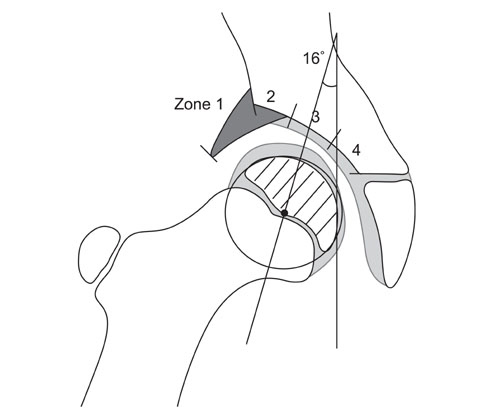
Fig. 2 Determination of the zone of compressive force (ZCF). The superior portion of the bony acetabulum is subdivided into three equal zones (numbered 2, 3, and 4); the portion of the roof consisting of the labrum alone is zone 1. ZCF is the acetabular zone which is entered by a line, tilted medially at 16° off the vertical (the vertical is a line perpendicular to the line of Hilgenreiner) and passing through the center of the femoral head. The circle is the smallest one that will completely contain the outer margin of the bony head; the point in the circle is its center. The figure shows a dysplastic hip in abduction; in such hips, the ZCF is usually zone 2 in the neutral position, shifting to zone 3 in abduction.
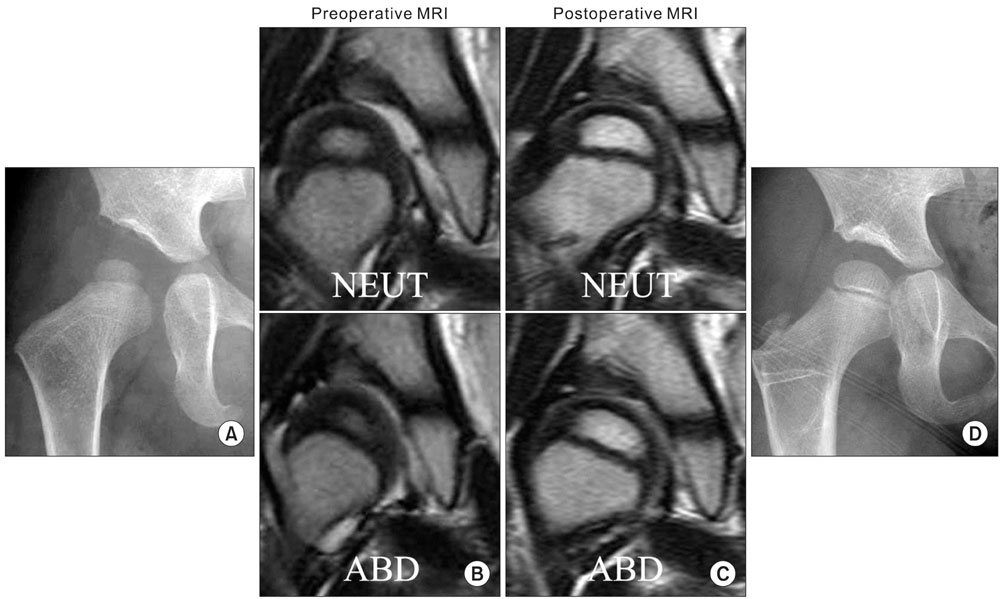
Fig. 3 Femoral osteotomy. (A) This 25-month-old girl had left hip dysplasia at initial presentation. (B) On the serial range of motion-magnetic resonance imaging (SROM-MRI), her uncorrected labral deformity (ULD) value was -3°; thus she was a candidate for a single femoral or pelvic osteotomy. Femoral varus osteotomy was performed when she was 29 months old. (C) After implant removal, she underwent a second SROM-MRI at 4 years and 2 months of age. Even though her ULD value following surgery was 3°, the zone of compressive force continued as zone 3 even in the neutral position (previously it was zone 2). (D) The radiograph, taken when he was 6 years and 2 months of age, showed improved condition of the hip. NEUT: neutral, ABD: abduction.

Fig. 4 Pelvic osteotomy. This boy had a right hip dislocation, and he underwent closed reduction when he was 13 months old. (A) At the age of 4 years and 5 months (3 years and 4 months after reduction), his right hip was still dysplastic. (B) On the serial range of motion-magnetic resonance imaging (SROM-MRI), the uncorrected labral deformity (ULD) value was 4° and the zone of compressive force (ZCF) shifted from zone 2 to 3; thus he was a candidate for single femoral or pelvic osteotomy. We performed a Salter innominate osteotomy when he was 4 years and 8 months old. (C) In a second SROM-MRI scan taken when he was 9 years and 1 month old, ZCF was zone 3 in both the neutral (NEUT) and abduction (ABD) positions and his ULD value was -6°. (D) The follow-up radiograph, taken at this time, showed improved condition of the hip.
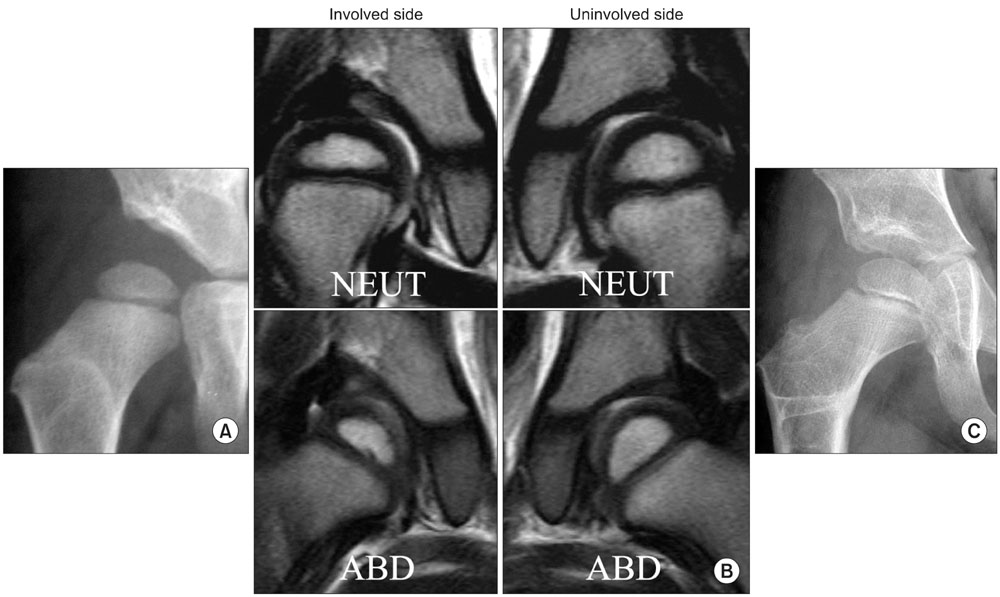
Fig. 5 Borderline case (single vs. dual osteotomy). This girl had a right hip dislocation, and she underwent closed reduction when she was 13 months old. (A) However, at the age of 4 years and 5 months, her right hip was still dysplastic. (B) On the serial range of motion-magnetic resonance imaging (SROM-MRI), her uncorrected labral deformity value was 6° and the zone of compressive force did not move medially on abduction, but remained at zone 2-3. Thus, we could have chosen to perform just one osteotomy (hip or pelvis) or both. To be on the safe side, we performed a dual femoral and pelvic osteotomy. (C) The follow-up radiograph, taken at the age of 9 years and 3 months, showed much improved condition of the hip. NEUT: neutral, ABD: abduction.
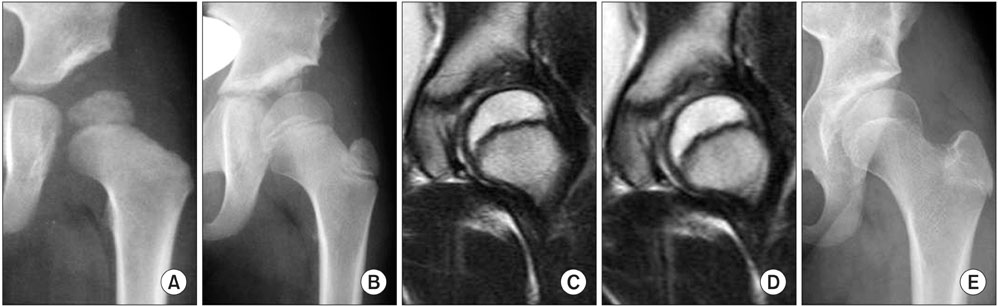
Fig. 6 Failure of unilateral osteotomy to reverse pathology. This girl had a left hip dislocation, and was treated with open reduction when she was 21 months old. (A) Two years after reduction (at 3 years and 9 months of age), the left hip was still dysplastic with a widened superior gap; at this time we performed a Dega-type periacetabular osteotomy. (B) Four years after the periacetabular osteotomy (at 7 years and 9 months of age), the left hip was still dysplastic and the superior gap was still wider than normal. At that time, the condition of the hip was checked by range of motion magnetic resonance imaging: (C) neutral and (D) abduction, which revealed a thickened medial acetabular wall and irregular ossification in the hypertrophied acetabular cartilage. (E) The final radiograph, taken at 13 years and 8 months of age, showed progress in the ossification at the widened superior joint gap, although it was not enough to lead to a normal hip joint (note the dysplasia, particularly the upward direction of the lateral end of the sourcil and the broken Shenton's line).
Reference
-
1. Mladenov K, Dora C, Wicart P, Seringe R. Natural history of hips with borderline acetabular index and acetabular dysplasia in infants. J Pediatr Orthop. 2002. 22(5):607–612.
Article2. Pirpiris M, Payman KR, Otsuka NY. The assessment of acetabular index: is there still a place for plain radiography? J Pediatr Orthop. 2006. 26(3):310–315.3. Tasnavites A, Murray DW, Benson MK. Improvement in acetabular index after reduction of hips with developmental dysplasia. J Bone Joint Surg Br. 1993. 75(5):755–759.
Article4. Tonnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976. (119):39–47.5. Wiberg G. Studies on dysplastic acetabular and congenital subluxation of the hip joint: with special reference to the complication of osteoarthritis. Parts HV. Acta Chir Scand Suppl. 1939. 83:Suppl 58. 7–38.6. Chen IH, Kuo KN, Lubicky JP. Prognosticating factors in acetabular development following reduction of developmental dysplasia of the hip. J Pediatr Orthop. 1994. 14(1):3–8.
Article7. Smith WS, Badgley CE, Orwig JB, Harper JM. Correlation of postreduction roentgenograms and thirty-one-year follow-up in congenital dislocation of the hip. J Bone Joint Surg Am. 1968. 50(6):1081–1098.
Article8. Wagner H. Weil UH, editor. Transplantation of the greater trochanter. Progress in orthopaedic surgery. Vol 2. Acetabular dyspasia and skeletal dysplasia in childhood. 1978. Heidelberga: Springer;99–102.9. Kim HT, Kim JI, Yoo CI. Acetabular development after closed reduction of developmental dislocation of the hip. J Pediatr Orthop. 2000. 20(6):701–708.
Article10. Ferguson SJ, Bryant JT, Ito K. The material properties of the bovine acetabular labrum. J Orthop Res. 2001. 19(5):887–896.
Article11. Horii M, Kubo T, Inoue S, Kim WC. Coverage of the femoral head by the acetabular labrum in dysplastic hips: quantitative analysis with radial MR imaging. Acta Orthop Scand. 2003. 74(3):287–292.
Article12. Kim YH. Acetabular dysplasia and osteoarthritis developed by an eversion of the acetabular labrum. Clin Orthop Relat Res. 1987. (215):289–295.
Article13. Miozzari HH, Clark JM, Jacob HA, von Rechenberg B, Notzli HP. Effects of removal of the acetabular labrum in a sheep hip model. Osteoarthritis Cartilage. 2004. 12(5):419–430.
Article14. Nishii T, Tanaka H, Sugano N, Miki H, Takao M, Yoshikawa H. Disorders of acetabular labrum and articular cartilage in hip dysplasia: evaluation using isotropic high-resolutional CT arthrography with sequential radial reformation. Osteoarthritis Cartilage. 2007. 15(3):251–257.
Article15. Petersen W, Petersen F, Tillmann B. Structure and vascularization of the acetabular labrum with regard to the pathogenesis and healing of labral lesions. Arch Orthop Trauma Surg. 2003. 123(6):283–288.
Article16. Ponseti IV. Morphology of the acetabulum in congenital dislocation of the hip: gross, histological and roentgenographic studies. J Bone Joint Surg Am. 1978. 60(5):586–599.
Article17. Ueshima K, Takahashi KA, Fujioka M, et al. Relationship between acetabular labrum evaluation by using radial magnetic resonance imaging and progressive joint space narrowing in mild hip dysplasia. Magn Reson Imaging. 2006. 24(5):645–650.
Article18. Pauwels F. Schatzker J, editor. Biomechanical principles of varus/valgus intertrochanteric osteotomy (Pauwels I and II) in the treatment of osteoarthritis of the hip. The intertrochanteric osteotomy. 1984. New York: Springer;3–23.
Article19. Albinana J, Morcuende JA, Weinstein SL. The teardrop in congenital dislocation of the hip diagnosed late: a quantitative study. J Bone Joint Surg Am. 1996. 78(7):1048–1055.
Article20. Albinana J, Dolan LA, Spratt KF, Morcuende J, Meyer MD, Weinstein SL. Acetabular dysplasia after treatment for developmental dysplasia of the hip: implications for secondary procedures. J Bone Joint Surg Br. 2004. 86(6):876–886.21. Brougham DI, Broughton NS, Cole WG, Menelaus MB. The predictability of acetabular development after closed reduction for congenital dislocation of the hip. J Bone Joint Surg Br. 1988. 70(5):733–736.
Article22. Harris NH, Lloyd-Roberts GC, Gallien R. Acetabular development in congenital dislocation of the hip: with special reference to the indications for acetabuloplasty and pelvic or femoral realignment osteotomy. J Bone Joint Surg Br. 1975. 57(1):46–52.23. Harris NH. Acetabular growth potential in congenital dislocation of the hip and some factors upon which it may depend. Clin Orthop Relat Res. 1976. (119):99–106.
Article24. Lindstrom JR, Ponseti IV, Wenger DR. Acetabular development after reduction in congenital dislocation of the hip. J Bone Joint Surg Am. 1979. 61(1):112–118.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pediatric Hip Disease (I): Diagnosis and Treatment of Developmental Dysplasia of the Hip
- Pediatric Hip Disease (II): Developmental Dysplasia of the Hip – Treatment of Residual Dysplasia
- Dynamic ultrasonography in developmental dysplasia of the hip treated with Pavlik harness
- Radiographic parameters of acetabulum for dysplasia in Korean adults
- Correlations between ultrasonographic and subsequent radiographic findings of developmental dysplasia of the hips
