J Korean Med Sci.
2004 Apr;19(2):229-233. 10.3346/jkms.2004.19.2.229.
Bone Marrow is Involved in Less than 10% of Patients with Nasal-Type NK/T Cell Lymphoma at Initial Diagnosis
- Affiliations
-
- 1Department of Pathology, Samsung Medical Center, Sungkyunkwan University, School of Medicine, Seoul, Korea. yhko@smc.samsung.co.kr
- KMID: 1733482
- DOI: http://doi.org/10.3346/jkms.2004.19.2.229
Abstract
- To evaluate the frequency of bone marrow involvement by nasal-type NK/T cell lymphoma, we retrospectively studied biopsy specimens from 40 patients by EBV in situ hybridization (ISH). Three patients had marrow involvement at initial diagnosis (7.5%). In one patient (1/40, 2.5%), the disease in bone marrow was recognized by routine morphological assessment, while two other patients had minimal involvement of lymphoma cells which was recognized only by EBV in situ hybridization (2/40, 5%). Two patients had a disseminated disease at diagnosis and died 6 days and 214 days after diagnosis. One patient had diffuse colonic lesion and died 82 days later. In conclusion, marrow involvement in nasal NK/T cell lymphoma is infrequent at initial diagnosis, and EBV ISH is a useful technique for identifying the minor subgroup of patients which have easily overlooked neoplastic involvement.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Biopsy
Bone Marrow/*pathology
Epstein-Barr Virus Infections/complications/pathology
Female
Herpesvirus 4, Human/genetics
Human
Killer Cells, Natural/*pathology
Lymphoma, T-Cell/complications/*pathology
Male
Middle Aged
Nasal Cavity/*pathology/virology
Prognosis
RNA, Viral/analysis
Retrospective Studies
Figure
-
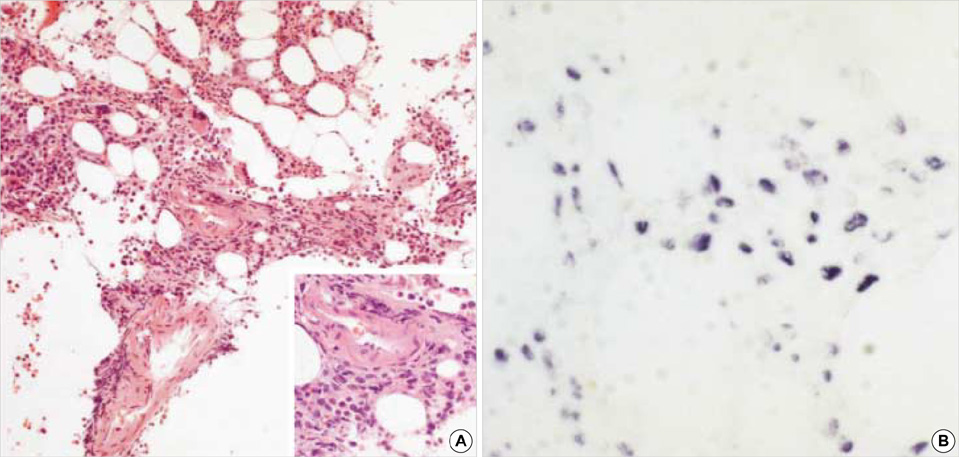
Fig. 1 Case 2 showing bone marrow involvement by NK/T cell lymphoma, which is identified by HE stain (A) as well as by EBV in-situ hybridization (B).

Fig. 2 Case No. 20. NK/T cell lymphoma in bone marrow is not suspected by H&E stain (A) and immunohistochemical stain with CD 3 (B) and CD56 (C), but detected by EBER in-situ hybridization (D).
Reference
-
1. Tumours of haematopoietic and lymphoid tissues. 2001. Lyon, France: IARC Press.2. Wong KF, Chan JK, Cheung MM, So JC. Bone marrow involvement by nasal NK cell lymphoma at diagnosis is uncommon. Am J Clin Pathol. 2001. 115:266–270.
Article3. Cheung MM, Chan JKC, Lau WH, Foo W, Chan PT, Ng CS, Ngan RK. Primary non-Hodgkin's lymphoma of the nose and nasopharynx: clinical features, tumor immunophenotype, and treatment outcome in 113 patients. J Clin Oncol. 1998. 16:70–77.
Article4. Kwong YL, Chan AC, Liang R, Chiang AK, Chim CS, Chan TK, Todd D, Ho FC. CD56+ NK lymphomas: clinicopathological features and prognosis. Br J Haematol. 1997. 97:821–829.5. Chinen K, Kaneko Y, Izumo T, Ohkura Y, Matsubara O, Tsuchiya E. Nasal natural killer cell/T-cell lymphoma showing cellular morphology mimicking normal lymphocytes. Arch Pathol Lab Med. 2002. 126:602–605.
Article6. Chan JK, Yip TT, Tsang WY, Ng CS, Lau WH, Poon YF, Wong CC, Ma VW. Detection of Epstein-Barr viral RNA in malignant lymphoma of the upper aerodigestive tract. Am J Surg Pathol. 1994. 18:938–946.7. Quintanilla-Martinez L, Franklin JL, Guerrero I, Krenacs L, Naresh KN, Rama-Rao C, Bhatia K, Raffeld M, Magrath IT. Histological and immunophenotypic profile of nasal NK/T cell lymphomas from Peru: high prevalence of p53 overexpression. Hum Pathol. 1999. 30:849–855.
Article8. Van Gorp J, Weiping L, Jacobse K, Liu YH, Li FY, De Weger RA, Li G. Epstein-Barr virus in nasal T-cell lymphomas (polymorphic reticulosis/midline malignant reticulosis) in western China. J Pathol. 1994. 173:81–87.
Article9. Tao Q, Ho FC, Loke SL, Srivastava G. Epstein-Barr virus is localized in the tumour cells of nasal lymphoma of NK, T or B cell type. Int J Cancer. 1995. 60:315–320.10. Sin LLP, Chan JKC, Kwong YL. Natural killer cell malignancies: clinicopathologic and molecular features. Histol Histopathol. 2002. 17:539–554.11. Ko YH, Ree HJ, Kim WS, Choi WH, Moon WS, Kim SW. Clinicopathologic and genotypic study of extranodal nasal-type natural killer/T-cell lymphoma and natural killer precursor lymphoma among Koreans. Cancer. 2000. 15:2106–2116.
Article12. The Non-Hodgkin's Lymphoma Classification Project. A clinical evaluation of the International Lymphoma Study Group Classification of non-Hodgkin's lymphoma. Blood. 1997. 89:3909–3918.13. Gaulard P, Kanavaros P, Farcet JP, Rocha FD, Haioun C, Divine M, Reyes F, Zafrani ES. Bone marrow histologic and immunohistochemical findings in peripheral T cell lymphoma: a study of 38 cases. Hum Pathol. 1991. 22:331–338.14. Fraga M, Brousset P, Schlaifer D, Payen C, Robert A, Rubie H, Huguet-Rigal F, Delsol G. Bone marrow involvement in anaplastic large cell lymphoma: immunohistochemical detection of minimal disease and its progonostic significance. Am J Clin Pathol. 1995. 103:82–89.15. Wong KF, Chan JK, Lo ES, Wong CS. A study of the possible etiologic association of Epstein-Barr virus with reactive hemophagocytic syndrome in Hong Kong Chinese. Hum Pathol. 1996. 27:1239–1242.
Article16. Carbone PP, Kaplan HS, Musshoff K, Smithers DW, Tubiana M. Report of the committee on Hodgkin's disease staging classification. Cancer Res. 1971. 31:1860–1861.17. Choe WH, Kim YH, Kim BJ, Lee JU, Lee JH, Son HJ, Rhee PL, Kim JJ, Paik SW, Rhee JC, Ko YH, Lee WY, Chun HK. The different colonoscopic manifestations of primary colorectal lymphomas by their cellular origin. Intestinal Res. 2003. 1:22–30. (in Korean).
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Extranodall NK/T-cell Lymphoma, Nasal type
- A Case of Aggressive T/NK-cell Lymphoma/leukemia with Cutaneous Involvement
- A Case of Coincident Multiple Myeloma and Nasal NK/T-Cell Lymphoma
- A Case of Primary Nasal CD56+ NK/T cell Lymphoma with Cutaneous Involvement
- Extranodal NK/T Cell Lymphoma, Nasal Type that Occurred in Patients with Atrophic Rhinitis
