Serial Micro-CT Assessment of the Therapeutic Effects of Rosiglitazone in a Bleomycin-Induced Lung Fibrosis Mouse Model
- Affiliations
-
- 1Department of Radiology, Research Institute of Clinical Medicine of Chonbuk National University, Biomedical Research Institute of Chonbuk National University Hospital, Institute for Medical Sciences, Jeonju 561-712, Korea. gyjin@chonbuk.ac.kr
- 2Department of Pathology, Research Institute of Clinical Medicine of Chonbuk National University, Biomedical Research Institute of Chonbuk National University Hospital, Institute for Medical Sciences, Jeonju 561-712, Korea.
- 3Department of Preventive Medicine, Research Institute of Clinical Medicine of Chonbuk National University, Biomedical Research Institute of Chonbuk National University Hospital, Institute for Medical Sciences, Jeonju 561-712, Korea.
- KMID: 1731048
- DOI: http://doi.org/10.3348/kjr.2014.15.4.448
Abstract
OBJECTIVE
The aim of this study was to assess the therapeutic effects of rosiglitazone with serial micro-CT findings before and after rosiglitazone administration in a lung fibrosis mouse model induced with bleomycin.
MATERIALS AND METHODS
We instilled the bleomycin solution directly into the trachea in twenty mice (female, C57BL/6 mice). After the instillation with bleomycin, mice were closely observed for 3 weeks and then all mice were scanned using micro-CT without sacrifice. At 3 weeks, the mice were treated with rosiglitazone on days 21 to 27 if they had abnormal CT findings (n = 9, 45%). For the mice treated with rosiglitazone, we performed micro-CT with mouse sacrifice 2 weeks after the rosiglitazone treatment completion. We assessed the abnormal CT findings (ground glass attenuation, consolidation, bronchiectasis, reticular opacity, and honeycombing) using a five-point scale at 3 and 6 weeks using Wilcoxon-signed ranked test. The micro-CT findings were correlated with the histopathologic results.
RESULTS
One out of nine (11.1%) mice improved completely. In terms of consolidation, all mice (100%) showed marked decrease from 3.1 +/- 1.4 at 3 weeks to 0.9 +/- 0.9 at 6 weeks (p = 0.006). At 6 weeks, mild bronchiectasis (n = 6, 66.7%), mild reticular opacity (n = 7, 77.8%) and mild honeycomb patterns (n = 3, 33.3%) appeared.
CONCLUSION
A serial micro-CT enables the evaluation of drug effects in a lung fibrosis mouse model.
Keyword
MeSH Terms
Figure
-
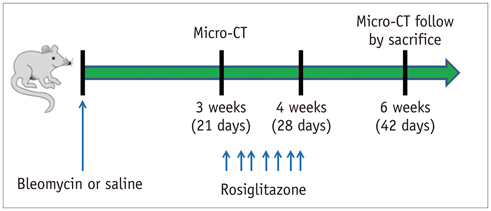
Fig. 1 Schematic diagram of experimental protocol. Control mice were instilled with saline into both lungs through tracheal cannula. In experimental group, bleomycin solution (60 µL as single dose) was instilled directly into trachea. Micro-CT was performed 3 weeks after instillation of bleomycin. When mice showed abnormal findings on micro-CT, rosiglitazone (5 mg/kg body weight/day) dissolved in distilled water was delivered seven times by oral gavage with 24-hour interval from days 21 to 27. Micro-CT was performed in mice treated with rosiglitazone to define effects of agent on lung 2 weeks after completion of rosiglitazone treatment.

Fig. 2 Mouse lung imaging performed using micro-CT scanner. Micro-CT image is provided with ruler which is generated by scanner system.

Fig. 3 Example of scoring of severity of consolidation on micro-CT. Severity of findings on imaging before and after rosiglitazone instillation in bleomycin-induced fibrosis mice model was semiquantitatively assessed on five-point scale. Consolidation was scored on 0 to 5 scale (absent = 0, less than 5% = 1, 5-25% = 2, 25-50% = 3, 50-75% = 4, more than 75% = 5) depending on area involved.

Fig. 4 Normal micro-CT finding of control mice. Micro-CTs of control mice show all normal findings at 3 and 6 weeks after intratracheal saline instillation.

Fig. 5 Case of improvement of lung fibrosis after administration of rosiglitazone shown on micro-CT. A. There is bilateral consolidation on micro-CT 3 weeks after bleomycin instillation. B. This is micro-CT image 6 weeks after bleomycin instillation. This mouse showed reduced bilateral consolidation, ground glass attenuation and bronchiectasis in same areas after administration of rosiglitazone. C. Interstitium is thickened by inflammatory cell infiltration on microscopy (hematoxylin and eosin stain, × 25).
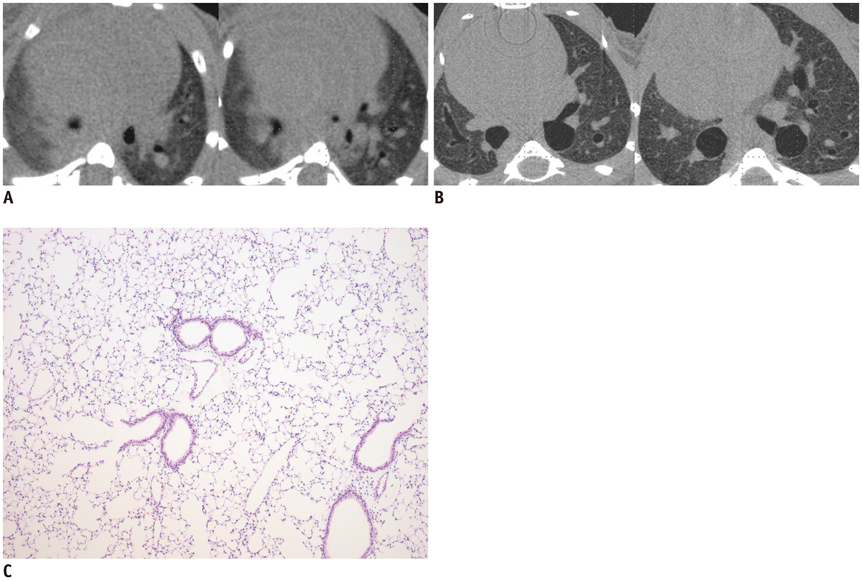
Fig. 6 Case of complete improvement of lung fibrosis after administration of rosiglitazone shown on micro-CT. A. There is diffuse peribronchial wall thickening, consolidation and ground glass attenuation on micro-CT 3 weeks after bleomycin instillation. B. This is micro-CT image 6 weeks after bleomycin instillation. Consolidation improved completely in same area 3 weeks after rosiglitazone treatment. C. There is minimal or no inflammatory cell infiltration in interstitium as seen on microscopy (hematoxylin and eosin stain, × 25).
Reference
-
1. Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011; 183:788–824.2. Peikert T, Daniels CE, Beebe TJ, Meyer KC, Ryu JH. Interstitial Lung Diseases Network of the American College of Chest Physicians. Assessment of current practice in the diagnosis and therapy of idiopathic pulmonary fibrosis. Respir Med. 2008; 102:1342–1348.3. Aono Y, Ledford JG, Mukherjee S, Ogawa H, Nishioka Y, Sone S, et al. Surfactant protein-D regulates effector cell function and fibrotic lung remodeling in response to bleomycin injury. Am J Respir Crit Care Med. 2012; 185:525–536.4. Yamashita CM, Dolgonos L, Zemans RL, Young SK, Robertson J, Briones N, et al. Matrix metalloproteinase 3 is a mediator of pulmonary fibrosis. Am J Pathol. 2011; 179:1733–1745.5. Genovese T, Cuzzocrea S, Di Paola R, Mazzon E, Mastruzzo C, Catalano P, et al. Effect of rosiglitazone and 15-deoxy-Delta12,14-prostaglandin J2 on bleomycin-induced lung injury. Eur Respir J. 2005; 25:225–234.6. Lakatos HF, Thatcher TH, Kottmann RM, Garcia TM, Phipps RP, Sime PJ. The Role of PPARs in Lung Fibrosis. PPAR Res. 2007; 2007:71323.7. Jin GY, Bok SM, Han YM, Chung MJ, Yoon KH, Kim SR, et al. Effectiveness of rosiglitazone on bleomycin-induced lung fibrosis: assessed by micro-computed tomography and pathologic scores. Eur J Radiol. 2012; 81:1901–1906.8. Langheinrich AC, Leithäuser B, Greschus S, Von Gerlach S, Breithecker A, Matthias FR, et al. Acute rat lung injury: feasibility of assessment with micro-CT. Radiology. 2004; 233:165–171.9. Ritman EL. Micro-computed tomography-current status and developments. Annu Rev Biomed Eng. 2004; 6:185–208.10. Johnson KA. Imaging techniques for small animal imaging models of pulmonary disease: micro-CT. Toxicol Pathol. 2007; 35:59–64.11. Ford NL, Wheatley AR, Holdsworth DW, Drangova M. Optimization of a retrospective technique for respiratory-gated high speed micro-CT of free-breathing rodents. Phys Med Biol. 2007; 52:5749–5769.12. Lee HJ, Goo JM, Kim NR, Kim MA, Chung DH, Son KR, et al. Semiquantitative measurement of murine bleomycin-induced lung fibrosis in in vivo and postmortem conditions using microcomputed tomography: correlation with pathologic scores--initial results. Invest Radiol. 2008; 43:453–460.13. Lee JA, Jin GY, Bok SM, Han YM, Park SJ, Lee YC, et al. Utility of micro CT in a murine model of bleomycin-induced lung fibrosis. Tuberc Respir Dis. 2009; 67:436–444.14. Burgess HA, Daugherty LE, Thatcher TH, Lakatos HF, Ray DM, Redonnet M, et al. PPARgamma agonists inhibit TGF-beta induced pulmonary myofibroblast differentiation and collagen production: implications for therapy of lung fibrosis. Am J Physiol Lung Cell Mol Physiol. 2005; 288:L1146–L1153.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Utility of Micro CT in a Murine Model of Bleomycin-Induced Lung Fibrosis
- Deficiency of Sphingosine-1-Phosphate Receptor 2 (S1Pâ‚‚) Attenuates Bleomycin-Induced Pulmonary Fibrosis
- Induction of Animal Model of Scleroderma with Repeated Injection of Bleomycin
- Effects of aging on accompanying intermittent hypoxia in a bleomycin-induced pulmonary fibrosis mouse model
- A Case of Bleomycin Induced Bronchiolitis Obliterans Orgnizing Pneumonia
