Yonsei Med J.
2011 Jul;52(4):595-602. 10.3349/ymj.2011.52.4.595.
A More Appropriate Cardiac Troponin T Level That Can Predict Outcomes in End-Stage Renal Disease Patients with Acute Coronary Syndrome
- Affiliations
-
- 1Department of Internal Medicine, School of Medicine, Ewha Womans University, Seoul, Korea. kbchoi@ewha.ac.kr
- 2Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1727991
- DOI: http://doi.org/10.3349/ymj.2011.52.4.595
Abstract
- PURPOSE
Cardiac troponin T (cTnT), a useful marker for diagnosing acute myocardial infarction (AMI) in the general population, is significantly higher than the usual cut-off value in many end-stage renal disease (ESRD) patients without clinically apparent evidence of AMI. The aim of this study was to evaluate the clinical usefulness of cTnT in ESRD patients with acute coronary syndrome (ACS).
MATERIALS AND METHODS
Two hundred eighty-four ESRD patients with ACS were enrolled between March 2002 and February 2008. These patients were followed until death or June 2009. Medical records were reviewed retrospectively. The cut-off value of cTnT for AMI was evaluated using a receiver operating characteristic (ROC) curve. We calculated Kaplan-Meier survival curves, and potential outcome predictors were determined by Cox proportional hazard analysis.
RESULTS
AMIs were diagnosed in 40 patients (14.1%). The area under the curve was 0.98 in the ROC curve (p<0.001; 95% CI, 0.95-1.00). The summation of sensitivity and specificity was highest at the initial cTnT value of 0.35 ng/mL (sensitivity, 0.95; specificity, 0.97). Survival analysis showed a statistically significant difference in all-cause and cardiovascular mortalities for the group with an initial cTnT > or =0.35 ng/mL compared to the other groups. Initial serum cTnT concentration was an independent predictor for mortality.
CONCLUSION
Because ESRD patients with an initial cTnT concentration > or =0.35 ng/mL have a poor prognosis, it is suggested that urgent diagnosis and treatment be indicated in dialysis patients with ACS when the initial cTnT levels are > or =0.35 ng/mL.
MeSH Terms
Figure
-
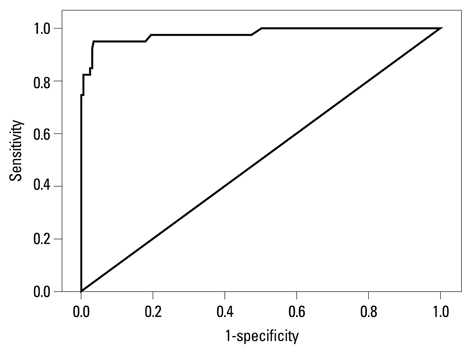
Fig. 1 Receiver operator characteristic (ROC) curve of cardiac troponin T (cTnT) for diagnosing acute myocardial infarction. The area under the curve (AUC) was 0.98 (p<0.001; 95% CI, 0.95-1.00). The cTnT value of 0.35 ng/mL offers the best overall sensitivity and specificity; the sensitivity was 0.95 and the specificity was 0.97.
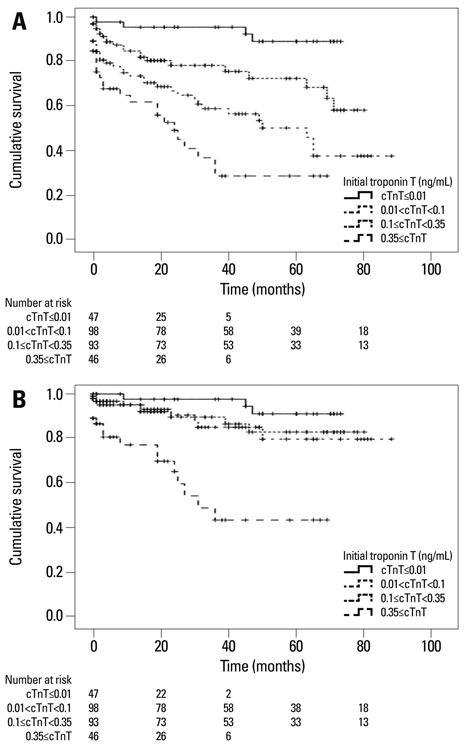
Fig. 2 Kaplan-Meier survival curves according to initial cardiac troponin T (cTnT) levels. (A) The all-cause mortality rate in the group with initial cTnT ≥0.35 ng/mL is significantly higher compared to the other groups by log-rank test (p<0.001). (B) The cardiovascular mortality rate in the group with initial cTnT ≥0.35 ng/mL is also significantly higher than in the other groups (p<0.001).
Reference
-
1. Farias MA, McClellan W, Soucie JM, Mitch WE. A prospective comparison of methods for determining if cardiovascular disease is a predictor of mortality in dialysis patients. Am J Kidney Dis. 1994. 23:382–388.
Article2. Parfrey PS, Foley RN. The clinical epidemiology of cardiac disease in chronic renal failure. J Am Soc Nephrol. 1999. 10:1606–1615.
Article3. Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003. 108:2154–2169.
Article4. Cheung AK, Sarnak MJ, Yan G, Berkoben M, Heyka R, Kaufman A, et al. Cardiac diseases in maintenance hemodialysis patients: results of the HEMO Study. Kidney Int. 2004. 65:2380–2389.
Article5. Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998. 32:S112–S119.
Article6. Joki N, Hase H, Nakamura R, Yamaguchi T. Onset of coronary artery disease prior to initiation of haemodialysis in patients with end-stage renal disease. Nephrol Dial Transplant. 1997. 12:718–723.
Article7. Collins AJ, Li S, Ma JZ, Herzog C. Cardiovascular disease in end-stage renal disease patients. Am J Kidney Dis. 2001. 38:S26–S29.
Article8. Sosnov J, Lessard D, Goldberg RJ, Yarzebski J, Gore JM. Differential symptoms of acute myocardial infarction in patients with kidney disease: a community-wide perspective. Am J Kidney Dis. 2006. 47:378–384.
Article9. Willging S, Keller F, Steinbach G. Specificity of cardiac troponins I and T in renal disease. Clin Chem Lab Med. 1998. 36:87–92.
Article10. McLaurin MD, Apple FS, Voss EM, Herzog CA, Sharkey SW. Cardiac troponin I, cardiac troponin T, and creatine kinase MB in dialysis patients without ischemic heart disease: evidence of cardiac troponin T expression in skeletal muscle. Clin Chem. 1997. 43:976–982.
Article11. Khan NA, Hemmelgarn BR, Tonelli M, Thompson CR, Levin A. Prognostic value of troponin T and I among asymptomatic patients with end-stage renal disease: a meta-analysis. Circulation. 2005. 112:3088–3096.
Article12. Aviles RJ, Askari AT, Lindahl B, Wallentin L, Jia G, Ohman EM, et al. Troponin T levels in patients with acute coronary syndromes, with or without renal dysfunction. N Engl J Med. 2002. 346:2047–2052.
Article13. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000. 36:959–969.
Article14. Wu AH, Valdes R Jr, Apple FS, Gornet T, Stone MA, Mayfield-Stokes S, et al. Cardiac troponin-T immunoassay for diagnosis of acute myocardial infarction. Clin Chem. 1994. 40:900–907.
Article15. Apple FS, Wu AH, Jaffe AS. European Society of Cardiology and American College of Cardiology guidelines for redefinition of myocardial infarction: how to use existing assays clinically and for clinical trials. Am Heart J. 2002. 144:981–986.
Article16. Apple FS, Murakami MM, Pearce LA, Herzog CA. Predictive value of cardiac troponin I and T for subsequent death in end-stage renal disease. Circulation. 2002. 106:2941–2945.
Article17. Freda BJ, Tang WH, Van Lente F, Peacock WF, Francis GS. Cardiac troponins in renal insufficiency: review and clinical implications. J Am Coll Cardiol. 2002. 40:2065–2071.18. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002. 106:2871–2872.
Article19. Diris JH, Hackeng CM, Kooman JP, Pinto YM, Hermens WT, van Dieijen-Visser MP. Impaired renal clearance explains elevated troponin T fragments in hemodialysis patients. Circulation. 2004. 109:23–25.
Article20. Soffer O, Fellner SK, Rush RL. Creatine phosphokinase in long-term dialysis patients. Arch Intern Med. 1981. 141:181–188.
Article21. McLaurin MD, Apple FS, Voss EM, Herzog CA, Sharkey SW. Cardiac troponin I, cardiac troponin T, and creatine kinase MB in dialysis patients without ischemic heart disease: evidence of cardiac troponin T expression in skeletal muscle. Clin Chem. 1997. 43:976–982.
Article22. Apple FS, Sharkey SW, Hoeft P, Skeate R, Voss E, Dahlmeier BA, et al. Prognostic value of serum cardiac troponin I and T in chronic dialysis patients: a 1-year outcomes analysis. Am J Kidney Dis. 1997. 29:399–403.
Article23. Kleiman NS, Lakkis N, Cannon CP, Murphy SA, DiBattiste PM, Demopoulos LA, et al. Prospective analysis of creatine kinase muscle-brain fraction and comparison with troponin T to predict cardiac risk and benefit of an invasive strategy in patients with non-ST-elevation acute coronary syndromes. J Am Coll Cardiol. 2002. 40:1044–1050.
Article24. Newby LK, Roe MT, Chen AY, Ohman EM, Christenson RH, Pollack CV Jr, et al. Frequency and clinical implications of discor dant creatine kinase-MB and troponin measurements in acute coronary syndromes. J Am Coll Cardiol. 2006. 47:312–318.
Article25. Dierkes J, Domrose U, Westphal S, Ambrosch A, Bosselmann HP, Neumann KH, et al. Cardiac troponin T predicts mortality in patients with end-stage renal disease. Circulation. 2000. 102:1964–1969.
Article26. Deegan PB, Lafferty ME, Blumsohn A, Henderson IS, McGregor E. Prognostic value of troponin T in hemodialysis patients is independent of comorbidity. Kidney Int. 2001. 60:2399–2405.
Article27. deFilippi C, Wasserman S, Rosanio S, Tiblier E, Sperger H, Tocchi M, et al. Cardiac troponin T and C-reactive protein for predicting prognosis, coronary atherosclerosis, and cardiomyopathy in patients undergoing long-term hemodialysis. JAMA. 2003. 290:353–359.
Article28. Havekes B, van Manen JG, Krediet RT, Boeschoten EW, Vandenbroucke JP, Dekker FW. NECOSAD Study Group. Serum troponin T concentration as a predictor of mortality in hemodialysis and peritoneal dialysis patients. Am J Kidney Dis. 2006. 47:823–829.
Article29. Jung HH, Ma KR, Han H. Elevated concentrations of cardiac troponins are associated with severe coronary artery calcification in asymptomatic haemodialysis patients. Nephrol Dial Transplant. 2004. 19:3117–3123.
Article30. Kontos MC, Garg R, Anderson FP, Tatum JL, Ornato JP, Jesse RL. Outcomes in patients admitted for chest pain with renal failure and troponin I elevations. Am Heart J. 2005. 150:674–680.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predictive Value of Cardiac Troponin I after Vascular Surgical Procedures
- The Long-Term Clinical Effects of Elevated Troponin during Percutaneous Coronary Intervention to Predict Long-Term Clinical Outcome in Patients with Acute Coronary Syndrome
- Acute Coronary Syndrome
- Diagnostic Value of Serum Cardiac Troponin T, Troponin I and CK-MB in Acute Kawasaki Disease
- Troponin assay use in the emergency department for management of patients with potential acute coronary syndrome: current use and future directions
