A Patient with Repeated Catastrophic Multi-Vessel Coronary Spasm after Zotarolimus-Eluting Stent Implantation
- Affiliations
-
- 1Department of Cardiology, Cardiovascular Center, Chonnam National University Hospital, Gwangju, Korea. cecilyk@hanmail.net
- KMID: 1723001
- DOI: http://doi.org/10.4070/kcj.2013.43.1.48
Abstract
- Drug-eluting stents (DES) have gained great popularity because of extraordinarily low rates of restenosis. Despite these superior clinical outcomes, several cases regarding the severe multi-vessel coronary spasm, although rare, after the placement of first generation DES have been reported. We report a case of severe, multi-vessel coronary spasm that occurred two occasions after placement of a zotarolimus-eluting stent, one of the second generation DES, in a 42-year-old man with unstable angina. The first incidence was relieved by intracoronary nitroglycerin alone, and second incident, which had combined fixed stenosis was treated with intracoronary nitroglycerin and everolimus-eluting stent.
Keyword
MeSH Terms
Figure
-
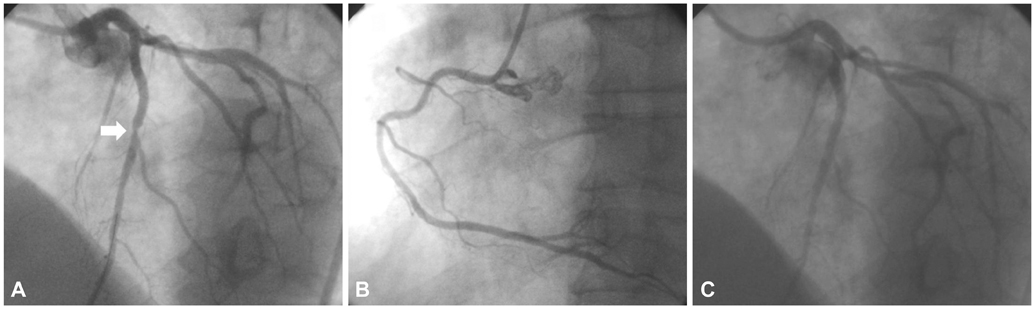
Fig. 1 Coronary angiogram at first admission. A: significant stenosis (arrow) in mid left anterior descending artery (LAD) (right anterior oblique cranial view). B: no significant stenosis in right coronary artery (left anterior oblique caudal view). C: good distal flow after drug-eluting stent implantation (2.75×18 mm Endeavor-R stent) in the mid LAD artery (right anterior oblique cranial view).
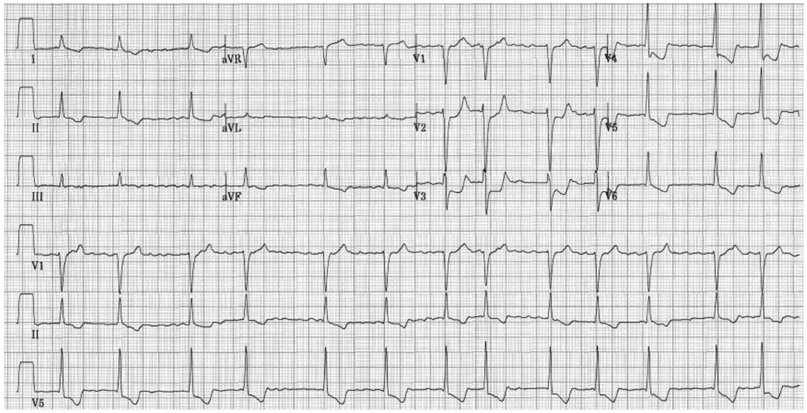
Fig. 2 Twelve-lead electrocardiogram showed atrial fibrillation and ST-segment elevation in lead aVR with ST-segment depression in multiple other leads, suggesting left main coronary artery disease.
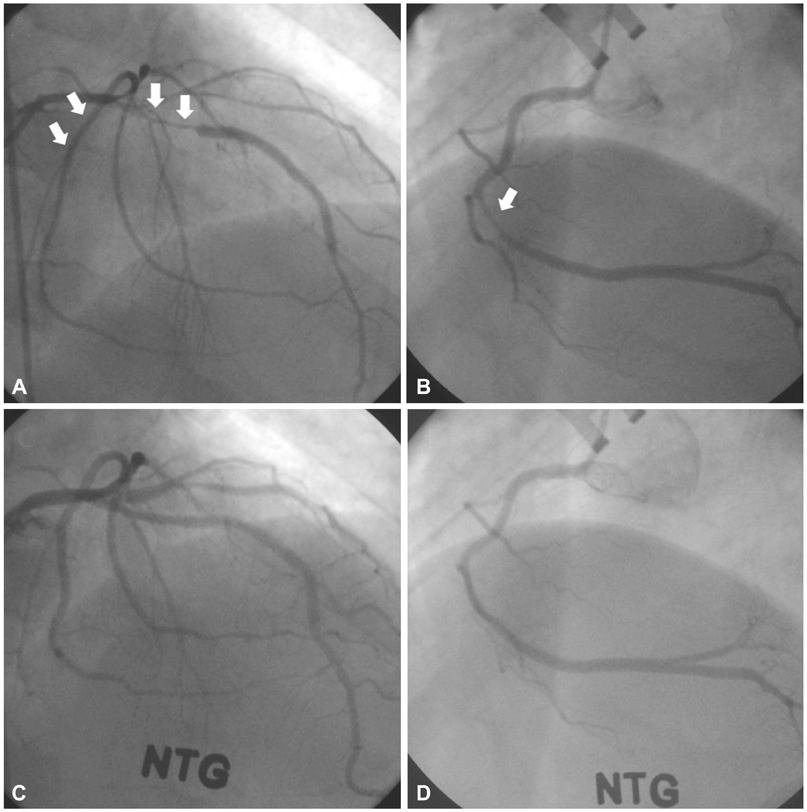
Fig. 3 Coronary angiogram at on second admission. A: spastic near total occlusion in proximal left anterior descending (LAD), proximal left circumflex artery (arrows) with a patent previously implanted stent in mid LAD (right anterior oblique cranial view). B: mid right coronary artery showing spastic near total occlusion (left anterior oblique caudal view) (arrow). C and D: the spasm was completely relieved by intracoronary nitroglycerin injection.
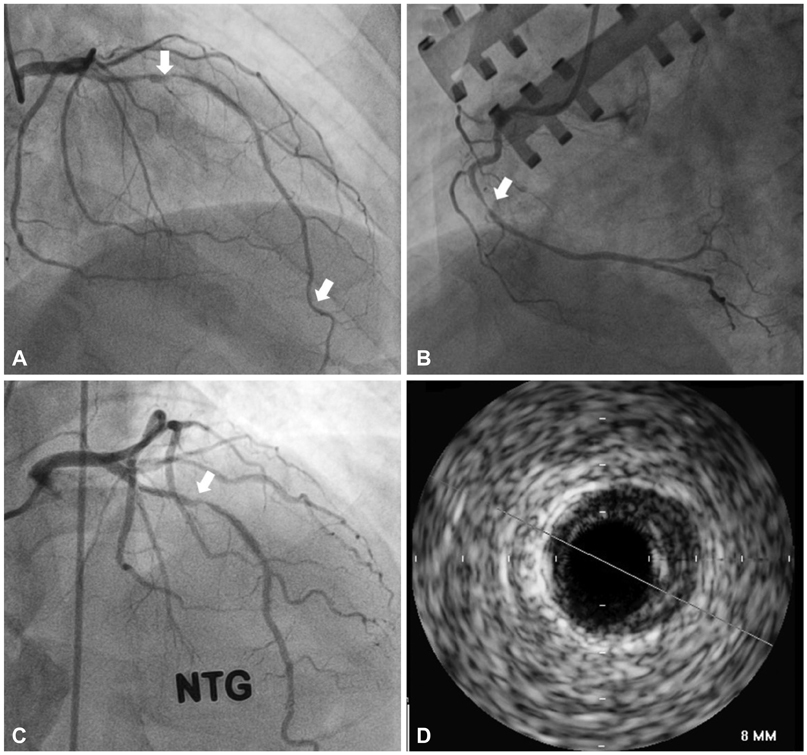
Fig. 4 CAG and IVUS at last admission (i.e., third admission). A: spasmodic stenosis in proximal and distal LAD (arrows). B: mid right coronary artery showing spasmodic stenosis (arrow). C: a repeat CAG after intracoronary administration of nitroglycerin demonstrated fixed stenosis in the proximal LAD at the proximal edge of the previously implanted zotarlimus-eluting stent (arrow). D: IVUS showing a large amount of plaque (minimal lumen area: 3.7 mm2, plaque burden: 55%). CAG: coronary angiography, IVUS: intravascular ultrasound, LAD: left anterior descending artery.
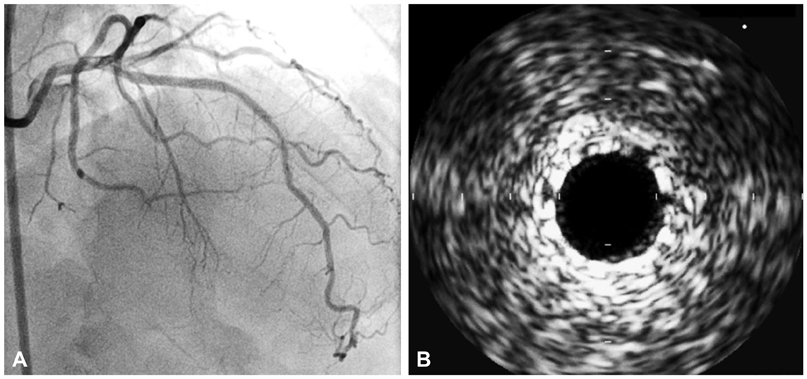
Fig. 5 Coronary angiogram (A) and intravascular ultrasound (B) after everolimus-eluting stent implantation (3.0×24 mm; Promus Element®, Boston Scientific, India). A: no residual stenosis with good distal flow. B: good stent apposition.
Reference
-
1. Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002. 346:1773–1780.2. Kounis NG, Kounis GN, Soufras GD. Kounis syndrome: a potential cause of simultaneous multivessel coronary spasm and thrombosis after drug-eluting stent implantation. J Invasive Cardiol. 2007. 19:200–201.3. Tomassini F, Varbella F, Gagnor A, Infantino V, Luceri S, Conte MR. Severe multivessel coronary spasm after sirolimus-eluting stent implantation. J Cardiovasc Med (Hagerstown). 2009. 10:485–488.4. Brott BC, Anayiotos AS, Chapman GD, Anderson PG, Hillegass WB. Severe, diffuse coronary artery spasm after drug-eluting stent placement. J Invasive Cardiol. 2006. 18:584–592.5. Togni M, Eberli FR. Vasoconstriction and coronary artery spasm after drug-eluting stent placement. J Invasive Cardiol. 2006. 18:593.6. Kim JW, Park CG, Seo HS, Oh DJ. Delayed severe multivessel spasm and aborted sudden death after Taxus stent implantation. Heart. 2005. 91:e15.7. Butt M, Connolly D, Lip GY. Drug-eluting stents: a comprehensive appraisal. Future Cardiol. 2009. 5:141–157.8. Togni M, Windecker S, Cocchia R, et al. Sirolimus-eluting stents associated with paradoxic coronary vasoconstriction. J Am Coll Cardiol. 2005. 46:231–236.9. Tan W, Cheng KL, Chen QX. Hypersensitivity to drug-eluting stent and stent thrombosis: Kounis or not Kounis syndrome? Chin Med J (Engl). 2009. 122:2390–2393.10. Suzuki T, Kopia G, Hayashi S, et al. Stent-based delivery of sirolimus reduces neointimal formation in a porcine coronary model. Circulation. 2001. 104:1188–1193.11. Byrne RA, Joner M, Kastrati A. Polymer coatings and delayed arterial healing following drug-eluting stent implantation. Minerva Cardioangiol. 2009. 57:567–584.12. Koh KK, Moon TH, Song JH, et al. Comparison of clinical and laboratory findings between patients with diffuse three-vessel coronary artery spasm and other types of coronary artery spasm. Cathet Cardiovasc Diagn. 1996. 37:132–139.13. Sugiishi M, Takatsu F. Cigarette smoking is a major risk factor for coronary spasm. Circulation. 1993. 87:76–79.14. Park YM, Han SH, Ko KP, et al. Diffuse multi-vessel coronary artery spasm: incidence and clinical prognosis. Int J Cardiol. 2012. [Epub ahead of print].15. Chuang YT, Ueng KC. Spontaneous and simultaneous multivessel coronary spasm causing multisite myocardial infarction, cardiogenic shock, atrioventricular block, and ventricular fibrillation. Circ J. 2009. 73:1961–1964.16. Kusama Y, Kodani E, Nakagomi A, et al. Variant angina and coronary artery spasm: the clinical spectrum, pathophysiology, and management. J Nippon Med Sch. 2011. 78:4–12.17. Miyagi H, Yasue H, Okumura K, Ogawa H, Goto K, Oshima S. Effect of magnesium on anginal attack induced by hyperventilation in patients with variant angina. Circulation. 1989. 79:597–602.18. Teragawa H, Kato M, Yamagata T, Matsuura H, Kajiyama G. The preventive effect of magnesium on coronary spasm in patients with vasospastic angina. Chest. 2000. 118:1690–1695.19. Motoyama T, Kawano H, Kugiyama K, et al. Vitamin E administration improves impairment of endothelium-dependent vasodilation in patients with coronary spastic angina. J Am Coll Cardiol. 1998. 32:1672–1679.20. Yasue H, Mizuno Y, Harada E, et al. Effects of a 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor, fluvastatin, on coronary spasm after withdrawal of calcium-channel blockers. J Am Coll Cardiol. 2008. 51:1742–1748.21. Park YM, Kang WC, Shin KC, et al. Repeated sudden cardiac death in coronary spasm: is IVUS helpful to decide treatment strategy? Int J Cardiol. 2012. 154:e57–e59.22. Kwon TG, Bae JH, Jeong MH, et al. N-terminal pro-B-type natriuretic peptide is associated with adverse short-term clinical outcomes in patients with acute ST-elevation myocardial infarction underwent primary percutaneous coronary intervention. Int J Cardiol. 2009. 133:173–178.23. Nebeker JR, Virmani R, Bennett CL, et al. Hypersensitivity cases associated with drug-eluting coronary stents: a review of available cases from the Research on Adverse Drug Events and Reports (RADAR) project. J Am Coll Cardiol. 2006. 47:175–181.24. Joner M, Nakazawa G, Finn AV, et al. Endothelial cell recovery between comparator polymer-based drug-eluting stents. J Am Coll Cardiol. 2008. 52:333–342.25. Sarno G, Lagerqvist B, Carlsson J, et al. Initial clinical experience with an everolimus eluting platinum chromium stent (Promus Element) in unselected patients from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). Int J Cardiol. 2012. [Epub ahead of print].
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Immediate Stent Fracture after Zotarolimus-Eluting Stent Implantation
- Simultaneous Multi-Vessel Subacute Stent Thromboses in Zotarolimus-Eluting Stents
- A Case of a Zotarolimus-Eluting Stent Fracture in the Left Anterior Descending Artery in a Patient Undergoing Hemodialysis
- A Case of Late Recurrent Vasospasm After Sirolimus-Eluting Stent Implantation
- Successful Management of a Rare Case of Stent Fracture and Subsequent Migration of the Fractured Stent Segment Into the Ascending Aorta in In-Stent Restenotic Lesions of a Saphenous Vein Graft
