Korean J Pediatr Infect Dis.
2014 Aug;21(2):150-156.
Neonatal Meningoencephalitis caused by Herpes Simplex Virus Type 2
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Korea. kjhan@catholic.ac.kr
- 2Vaccine Bio Research Institute, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Abstract
- Despite its rare occurrence, early diagnosis and appropriate treatment for neonatal herpes simplex virus infection are mandatory due to its high morbidity and mortality. In Korea, there has been no epidemiologic data on neonatal herpes simplex virus infection, and even case reports are rare. We observed a 16-day-old neonate who presented with fever and seizures. We diagnosed her with meningoencephalitis caused by herpes simplex virus type 2 based on the polymerase chain reaction test, and treated her with intravenous acyclovir and anticonvulsants. The seroprevalence of herpes simplex virus type 2 sharply increases in women in their 30s, and the average age for childbirth has increased to older than 30 years of age in Korea; we therefore expect that the incidence of neonatal herpes simplex virus type 2 infection will rise in Korea, and more attention should be directed to neonatal herpes simplex virus type 2 infection. We report this newborn patient's case along with a literature review.
MeSH Terms
Figure
-
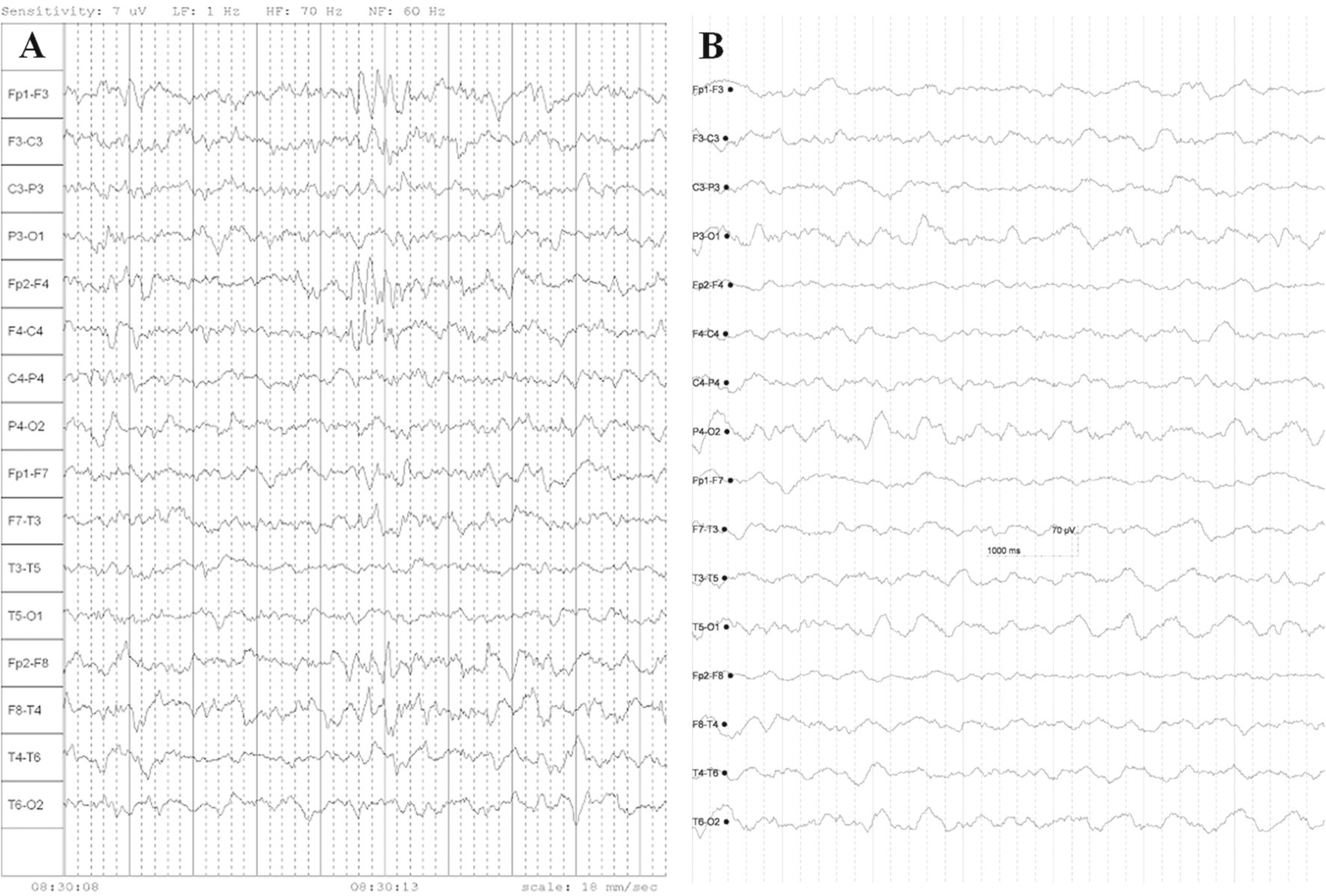
Fig. 1. (A) The initial electroencephalography shows regular and symmetric background activity of 1–3 Hz, with intermittent sharp high-amplitude waves in both frontal areas. (B) An EEG repeated at three months after diagnosis of meningoencephalitis shows no abnormal findings.

Fig. 2. (A) Initial brain magnetic resonance imaging on hospital day 2 shows only leptomeningeal enhancement on the axial T1-weighted image. Repeated brain magnetic resonance imaging three months after the diagnosis shows (B) cystic lesions in the cortex and subcortical white matter of both frontal lobes on the axial T1-weighted image and (C) old hemorrhages in the cerebral parenchyma and (D) the cerebellar parenchyma on the axial echo planar image.
Reference
-
References
1. Corey L, Wald A. Maternal and neonatal herpes simplex virus infections. N Engl J Med. 2009; 361:1376–85.
Article2. Whitley RJ, Nahmias AJ, Visintine AM, Fleming CL, Alford CA. The natural history of herpes simplex virus infection of mother and newborn. Pediatrics. 1980; 66:489–94.
Article3. Schleede L, Bueter W, Baumgartner-Sigl S, Opladen T, Weigt-Usinger K, Stephan S, et al. Pediatric herpes simplex virus encephalitis: a retrospective multicenter experience. J Child Neurol. 2013; 28:321–31.4. Long SS, Pool TE, Vodzak J, Daskalaki I, Gould JM. Herpes simplex virus infection in young infants during 2 decades of empiric acyclovir therapy. Pediatr Infect Dis J. 2011; 30:556–61.
Article5. Kim ID, Chang HS, Hwang KJ. Herpes simplex virus 2 infection rate and necessity of screening during pregnancy: a clinical and seroepidemiologic study. Yonsei Med J. 2012; 53:401–7.
Article6. Kucera P, Gerber S, Marques-Vidal P, Meylan PR. Seroepidemiology of herpes simplex virus type 1 and 2 in pregnant women in Switzerland: an obstetric clinic based study. Eur J Obstet Gynecol Reprod Biol. 2012; 160:13–7.
Article7. Xu F, Sternberg MR, Kottiri BJ, McQuillan GM, Lee FK, Nahmias AJ, et al. Trends in herpes simplex virus type 1 and type 2 seroprevalence in the United States. JAMA. 2006; 296:964–73.
Article8. Shin HS, Park JJ, Chu C, Song HJ, Cho KS, Lee JS, et al. Herpes simplex virus type 2 seroprevalence in Korea: rapid increase of HSV-2 seroprevalence in the 30s in the southern part. J Korean Med Sci. 2007; 22:957–62.
Article9. Statistics Korea. Korean Statistical Information Service. Available at. http://kosis.kr/statisticsList/statisticsList_01List.jsp?vwcd=MT_ZTITLE&parentId=A. [accessed on 1 November 2013].10. Corey L, Whitley RJ, Stone EF, Mohan K. Difference between herpes simplex virus type 1 and type 2 neonatal encephalitis in neurological outcome. Lancet. 1988; 331:1–4.
Article11. Whitley R, Arvin A, Prober C, Corey L, Burchett S, Plotkin S, et al. Predictors of morbidity and mortality in neonates with herpes simplex virus infections. The National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group. N Engl J Med. 1991; 324:450–4.12. Landry ML, Mullangi P, Nee P, Klein BR. Herpes simplex virus type 2 acute retinal necrosis 9 years after neonatal herpes. J Pediatr. 2005; 146:836–8.
Article13. Vossough A, Zimmerman RA, Bilaniuk LT, Schwartz EM. Imaging findings of neonatal herpes simplex virus type 2 encephalitis. Neuroradiology. 2008; 50:355–66.
Article14. Tiffany KF, Benjamin DK Jr, Palasanthiran P, O'Donnell K, Gutman LT. Improved neurodevelopmental outcomes following longterm high-dose oral acyclovir therapy in infants with central nervous system and disseminated herpes simplex disease. J Perinatol. 2005; 25:156–61.
Article15. Kimberlin DW, Whitley RJ, Wan W, Powell DA, Storch G, Ahmed A, et al. Oral acyclovir suppression and neurodevelopment after neonatal herpes. N Engl J Med. 2011; 365:1284–92.
Article16. Caviness AC, Demmler GJ, Swint JM, Cantor SB. Costeffectiveness analysis of herpes simplex virus testing and treatment strategies in febrile neonates. Arch Pediatr Adolesc Med. 2008; 162:665–74.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of neonatal herpes simplex virus encephalitis
- Herpes Meningoencephalitis Complicated by Cerebral Hematomas During Acyclovir Therapy
- A Case of Disseminated Herpes Simplex Virus Infection in Immunocompromised Patient
- Asymptomatic Hematoma in Herpes Simplex Encephalitis
- A Case of Chronic Herpes Simplex Virus Infection Misdiagnosed as a Perforating Dermatosis
