Tuberc Respir Dis.
2006 Apr;60(4):397-403. 10.4046/trd.2006.60.4.397.
Relationship between Dyspnea and Disease Severity, Quality of Life, and Social Factor in Patients with Chronic Obstructive Pulmonary Disease
- Affiliations
-
- 1Department of Internal Medicine, School of Medicine, Kyungpook National University, Korea. kimch@knu.ac.kr
- KMID: 1719364
- DOI: http://doi.org/10.4046/trd.2006.60.4.397
Abstract
-
BACKGROUND: Chronic obstructive pulmonary disease(COPD) is categorized by the percentage of the predicted FEV1(Forced expiratory volume in 1 second) result which is highly correlated with disease severity(morbidity and mortality). In COPD patients, dyspnea seems to be different from disease severity. We investigated whether dyspnea is correlated with disease severity, as measured by FEV1, quality of life(QoL), occupation, and supporting level of family members and neighbors.
METHOD: Thirty-six clinically stable patients with chronically irreversible airflow limitation were enrolled. We used the Medical Research Council(MRC) dyspnea scale to assess the level of dyspnea and the Korean St. Goerge's respiratory questionnaire(SGRQ) as measure the QoL.
RESULT: The mean percentage of the predicted FEV1 was 32.0%. Dyspnea was not correlated with GOLD stage using FEV1(p=0.114). With deteriorating level of dyspnea the scores of symptoms(p=0.041), activity(p=0.004), impact(p=0.001), and total SGRQ score(p<0.001) were significantly increased. Dyspnea was not correlated with the level of occupation(p=0.259). The supporting level of family members and neighbors was significantly negatively correlated with dyspnea scale(p=0.011).
CONCLUSION
In the management of COPD patients, we have to remember that the level of subjective dyspnea is correlated with QoL(symptom, activity and impact on society) and social supporting level as well as GOLD stage(FEV1).
Keyword
Figure
-

Figure 1 Relationship between SGRQ score and MRC dyspnea scale. *p<0.05 for comparison with patients with MRC scale 1& 2. †p<0.05 for comparison with patients with MRC scale 3. ‡p<0.05 for comparison with patients with MRC scale 4.
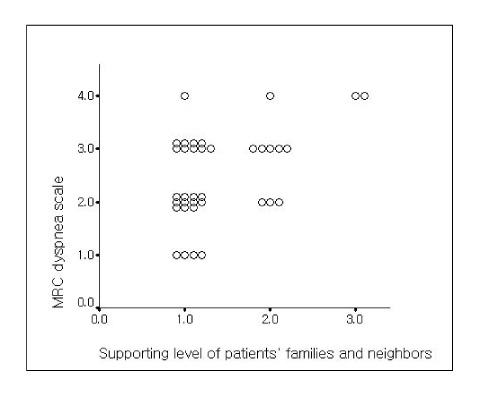
Figure 2 Relationship between MRC dyspnea scale and supporting level of patients' families and neighbors(p=0.011). For definition of class 1, 2 and 3, see the method of text.
Reference
-
1. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global initiative for chronic obstructive lung disease(COPD) Workshop summary. Am J Respir Crit Care Med. 2001. 163:1256–1276.2. Fabbri LM, Hurd SS. Global strategy for the diagnosis, management, and prevention of Chronic Obstructive Lung Disease: 2003 updated. Eur Respir J. 2003. 22:1–2.3. Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, et al. Harrison's principles of internal medicine. 2005. 16th ed. McGraw-Hill;201.4. Hajiro T, Nishimura K, Tsukino M, Ikeda A, Koyama H, Izumi T. Comparison of discriminative properties among disease-specific questionnaires for measuring heath-related quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998. 157:785–790.5. Wolkove N, Dajezman E, Colacone A, Kreisman H. The relationship between pulmonary function and dyspnea in obstructive lung disease. Chest. 1989. 96:1247–1251.6. Pearson MG, Bellamy D, Calverley PM, Honeybourne D, MacNee W, Rudolf M, et al. BTS guideline for the management of chronic obstructive pulmonary disease. Thorax. 1997. 52:Suppl. S1–S28.7. Cooper CB, Tashkin DP. Recent developments in inhaled therapy in stable chronic obstructive pulmonary disease. BMJ. 2005. 330:640–644.8. van der Molen T, Willemse BW, Schokker S, ten Hacken NH, Postma DS, Juniper EF. Development, validity and responsiveness of the Clinical COPD Questionnaire. Health Qual Life Outcomes. 2003. 1:13.9. Curtis JR, Martin DP, Martin TR. Patient-assessed health outcomes in chronic lung disease: what are they, how do they help us, and where do we go from here? Am J Respir Crit Care Med. 1997. 156:1032–1039.10. Curtis JR, Deyo RA, Hudson LD. Pulmonary rehabilitation in chronic respiratory insufficiency: 7. health-related quality of life among patients with chronic obstructive pulmonary disease. Thorax. 1994. 49:162–170.11. Mahler DA. How should health-related quality of life be assessed in patients with COPD? Chest. 2000. 117:54S–57S.12. Ferrer M, Alonso J, Morera J, Marrades RM, Khalaf A, Aguar MC, et al. Chronic obstructive pulmonary disease stage and health-related quality of life. Ann Intern Med. 1997. 127:1072–1079.13. Fletcher CM, Elmes PC, Fairbairn AS, Wood CH. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br Med J. 1959. (5147):257–266.14. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation: The St. George's Rsepiratory Questionnaire. Am Rev Respir Dis. 1992. 145:1321–1327.15. Jones PW, Quirk FH, Baveystock CM. The St. George's Respiratory Questionnaire. Respir Med. 1991. 85:Suppl B. 25–31.16. Williams SJ, Bury MR. Impairment, disability and handcap in chronic respiratory illness. Soc Sci Med. 1989. 29:609–616.17. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988. 93:580–586.18. Hajiro T, Nishimura K, Tsukino M, Ikeda A, Oga T, Izumi T. A comparison of the level of dyspnea vs disease severity in indicating the health-related quality of life of patients with COPD. Chest. 1999. 116:1632–1637.19. Okbadejo AA, Jones PW, Wedzicha JA. Quality of life in patients with chronic obstructive pulmonary disease and severe hypoxemia. Thorax. 1996. 51:44–47.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Quality of Life with the Chronic Obstructive Pulmonary Disease Assessment Test in Chronic Obstructive Pulmonary Disease and the Effect of Dyspnea on Disease-Specific Quality of Life in These Patients
- The Effects of Self-Efficacy Promoting Pulmonary Rehabilitation Program in Out-Patients with Chronic Obstructive Pulmonary Disease
- Pulmonary Rehabilitation in Chronic Obstructive Pulmonary Disease (COPD)
- Effects of Different Modes of Upper Limb Training in Individuals With Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
- Structural Equation Modeling on Successful Aging in Elders with Chronic Obstructive Pulmonary Disease Based on Selection-Optimization-Compensation Strategy
