Anococcygeal Raphe Revisited: A Histological Study Using Mid-Term Human Fetuses and Elderly Cadavers
- Affiliations
-
- 1Division of Colon and Rectal Surgery, Shizuoka Cancer Center Hospital, Shizuoka, Japan. y.kinugasa@scchr.jp
- 2Arakawa Clinic of Proctology, Tokyo, Japan.
- 3Department of Anatomy, Akita University School of Medicine, Akita, Japan.
- 4Oral Health Science Center hrc8, Tokyo Dental College, Chiba, Japan.
- 5Department of Surgery, Chonbuk National University School of Medicine, Jeonju, Korea.
- 6Division of Internal Medicine, Iwamizawa Kojin-kai Hospital, Iwamizawa, Japan.
- 7Department of Surgical Oncology, Graduate School, Tokyo Medical and Dental University, Tokyo, Japan.
- KMID: 1716888
- DOI: http://doi.org/10.3349/ymj.2012.53.4.849
Abstract
- PURPOSE
We recently demonstrated the morphology of the anococcygeal ligament. As the anococcygeal ligament and raphe are often confused, the concept of the anococcygeal raphe needs to be re-examined from the perspective of fetal development, as well as in terms of adult morphology.
MATERIALS AND METHODS
We examined the horizontal sections of 15 fetuses as well as adult histology. From cadavers, we obtained an almost cubic tissue mass containing the dorsal wall of the anorectum, the coccyx and the covering skin. Most sections were stained with hematoxylin and eosin or Masson-trichrome solution.
RESULTS
The adult ligament contained both smooth and striated muscle fibers. A similar band-like structure was seen in fetuses, containing: 1) smooth muscle fibers originating from the longitudinal muscle coat of the anal canal and 2) striated muscle fibers from the external anal sphincter (EAS). However, in fetuses, the levator ani muscle did not attach to either the band or the coccyx. Along and around the anococcygeal ligament, we did not find any aponeurotic tissue with transversely oriented fibers connecting bilateral levator ani slings. Instead, in adults, a fibrous tissue mass was located at a gap between bilateral levator ani slings; this site corresponded to the dorsal side of the ligament and the EAS in the immediately deep side of the natal skin cleft.
CONCLUSION
We hypothesize that a classically described raphe corresponds to the specific subcutaneous tissue on the superficial or dorsal side of the anococcygeal ligament.
Keyword
MeSH Terms
Figure
-

Fig. 1 Sagittal sections of the miadsagittal area including the coccyx (CO) and anococcygeal ligament. Masson trichrome staining. (A) 96 years old male, displays a thick external anal sphincter (EAS) in the 30 mm inferior side of the CO. (B) 84 years old female, exhibits a thin EAS 40 mm below the CO. The anococcygeal ligament (ACL) merges with the EAS as well as the longitudinal anal muscle (arrows) between the EAS and internal anal sphincter (IAS). Inserts in panels A and B are higher magnification views of a square in panel A or B, respectively. Insert in panel A shows smooth muscles in the ACL, while an inset in panel B striated muscles distributing in the inferior end of the ACL. Note a fibrous tissue (stars) in the dorsal side of the ligament. Asterisk in panel A (or in the insert in panel B) indicates the dorsosuperior reflection of the well developed EAS (or an artificial damage during the histological procedure).
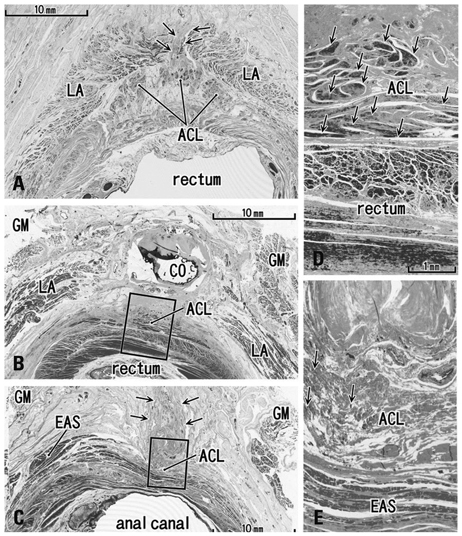
Fig. 2 Transverse sections of the anal canal dorsal wall. (A) 86 years old female, 10 mm inferior side of the coccyx (CO), displays a small fibrous tissue mass (arrows) at a gap between the bilateral levator slings (LA). This gap was the smallest in specimens examined (3 mm). (B) 92 years old male, inferior end of the CO and the most superior part of the anococcygeal ligament (ACL). (C) Same specimen as panel B. Panel B corresponds to the, whereas panel C contains the inferior end of the ligament at a level 20 mm inferior side of the CO. In panel C, note a fibrous tissue mass (arrows) in the dorsal side of the external anal sphincter (EAS) and the ligament. (D) A higher magnification view of a square in panel B. (E) A higher magnification view of a square in panel C. Arrows in panels D and E show smooth muscles (panel D) or striated muscles (panel E) in the anococcygeal ligament, respectively. GM, gluteus maximus muscle.
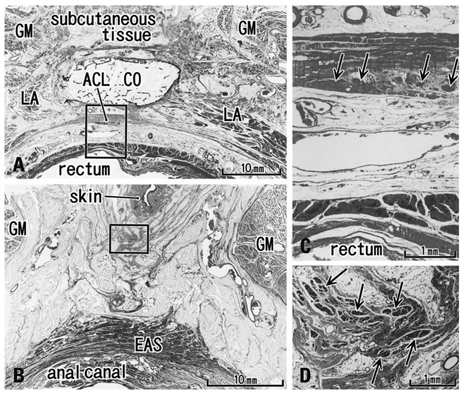
Fig. 3 Transverse sections of the anal canal and natal skin cleft (85 years old male). (A) A level of the inferior end of the coccyx (CO) contains the most superior part of the anococcygeal ligament (ACL). (B) A level 40 mm inferior side of the CO. A fibrous tissue extends between the natal cleft (skin) and the external anal sphincter (EAS). (C) A higher magnification view of a square in panel A. Arrows show smooth muscles in the ligament. (D) A higher magnification view of a square in panel B. Arrows show striated muscles in the subcutaneous fibrous tissue. LA, levator ani muscle; GM, gluteus maximus muscle.

Fig. 4 Horizontal sections of the anal canal in a 12-week fetus. (A) Immunohistochemistry for smooth muscle actin (SMA). 0.2 mm superior side of panel C. A dorsal midsagittal structure (arrows) is positive for SMA and extending from the longitudinal smooth muscle coat of the anal canal toward the coccyx (CO). (B) Immunohistochemistry for SMA. The dorsal extension (arrows) of the external anal sphincter (EAS). (C) Immunohistochemistry for desmin (a striated muscle marker) of a section near panel B. All panels are prepared at the same magnification (scale bar in panel A). COM, coccygeus muscle; IC, ishchiocavernosus muscle; OI, obturator internus muscle. PF, pelvic fascia.

Fig. 5 Tilted horizontal sections of the anal canal dorsal wall in a 20-week fetus. HE staining. (A) The most superior side of the figure includes the inferior end of the coccyx (CO). Lower magnification than other panels while panels B, C and D are at the same magnification (B) 0.2 mm inferior to the panel A. (C) 0.2 mm inferior to the panel B. (D) The most inferior side of the figure and 0.2 mm inferior to the panel C. The levator ani muscle is located out side of the figure (much more superior and lateral). A connective tissue mass (asterisk) is present in the dorsal side of the CO. In the inferior side of the CO (panels C and D), another connective tissue mass (star) is seen connecting to the CO. Panels C and D include the back skin in the upper side of each panel. Fatty tissues (fat) start development in the ventral side of the gluteus maximus muscle (GM). In this specimen, there is no specific structure connecting between the external anal sphincter (EAS) and the inferior elongation of the coccyx (star).
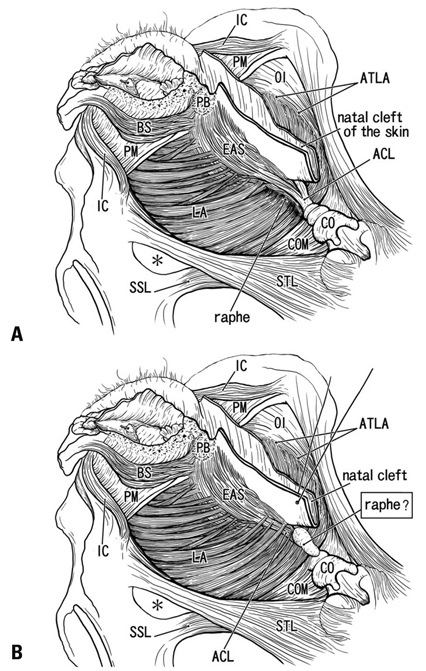
Fig. 6 Anococcygeal raphe: a classical concept and our identification according to the present histology. (A) A classical view of the anococcygeal raphe (raphe) in dorsal views of the female perineum. (B) Our identification according to the present study. Muscles are not drawn in a dorsal part of the ischorectal fossa (asterisk). In the diagram, the ventral part of the female perineum is drawn according to our recent studies.20,30 ACL, anococcygeal ligament; ATLA, arcus tendineus for the levator ani; BS, bulbospongiosus muscle; CO, coccyx; COM, coccygeus muscle; EAS, external anal sphincter; IC, ishchiocavernosus muscle; LA, levator ani; OI, obturator internus muscle; PB, perneal body; PM, perineal membrane; SSL, sacrospinous ligament; STL, sacrotuberous ligament.
Reference
-
1. Kinugasa Y, Arakawa T, Abe S, Ohtsuka A, Suzuki D, Murakami G, et al. Anatomical reevaluation of the anococcygeal ligament and its surgical relevance. Dis Colon Rectum. 2011. 54:232–237.
Article2. Bogduk N. Issues in anatomy: the external anal sphincter revisited. Aust N Z J Surg. 1996. 66:626–629.
Article3. Borley NR. Standring S, editor. Anal canal. Gray's Anatomy. 2008. 40 ed. London: Elsevier Churchill Linvingstone;1155–1160.4. Toldt BvC. Atlas of Human Anatomy for Students and Surgeons. 1903. Berlin: Urban & Schwarzenberg.5. Gräfenberg E. Development of the human pelvic musculature. Anat Hefte. 1904. 72:429–494.6. Bardeen RC. Development and variation of the musculature of the inferior extremity and the neighboring regions of the trunk in man. Am J Anat. 1907. 6:332–336.7. Power RM. Embryological development of the levator ani muscle. Am J Obstet Gynecol. 1948. 55:367–381.
Article8. Tichý M. The development and organization of the sphincter ani externus and the adjacent part of the levator ani muscle in man. Folia Morphol (Praha). 1984. 32:113–120.9. Fritsch H, Fröhlich B. Development of the levator ani muscle in human fetuses. Early Hum Dev. 1994. 37:15–25.
Article10. Fröber R, Krebs U, Haas A, Fischer MS, Schier F, Linss W. Three-dimensional reconstruction of the anal striated musculature in a human fetus. Cells Tissues Organs. 2001. 169:152–157.
Article11. Schier F, Krebs U, Fröber R, Haas A. Three-dimensional reconstruction of the anorectal continence organ in a 14-week-old fetus. J Pediatr Surg. 2002. 37:912–915.
Article12. Koch WF, Marani E. Early development of the human pelvic diaphragm. Adv Anat Embryol Cell Biol. 2007. 192:1–111.
Article13. Fritsch H. Developmental changes in the retrorectal region of the human fetus. Anat Embryol (Berl). 1988. 177:513–522.
Article14. Levi AC, Borghi F, Garavoglia M. Development of the anal canal muscles. Dis Colon Rectum. 1991. 34:262–266.
Article15. Niikura H, Jin ZW, Cho BH, Murakami G, Yaegashi N, Lee JK, et al. Human fetal anatomy of the coccygeal attachments of the levator ani muscle. Clin Anat. 2010. 23:566–574.
Article16. Hayashi S, Murakami G, Ohtsuka A, Itoh M, Nakano T, Fukuzawa Y. Connective tissue configuration in the human liver hilar region with special reference to the liver capsule and vascular sheath. J Hepatobiliary Pancreat Surg. 2008. 15:640–647.
Article17. Miyake N, Hayashi S, Kawase T, Cho BH, Murakami G, Fujimiya M, et al. Fetal anatomy of the human carotid sheath and structures in and around it. Anat Rec (Hoboken). 2010. 293:438–445.
Article18. Ayoub SF. The anterior fibres of the levator ani muscle in man. J Anat. 1979. 128(Pt 3):571–580.19. Ayoub SF. Anatomy of the external anal sphincter in man. Acta Anat (Basel). 1979. 105:25–36.
Article20. Kato M, Matsubara A, Murakami G, Abe S, Ide Y, Sato I, et al. Female perineal membrane: a study using pelvic floor semiserial sections from elderly nulliparous and multiparous women. Int Urogynecol J Pelvic Floor Dysfunct. 2008. 19:1663–1670.
Article21. Arakawa T, Hayashi S, Kinugasa Y, Murakami G, Fujimiya M. Development of the external anal sphincter with special reference to intergender difference: observations of mid-term fetuses (15-30 weeks of gestation). Okajimas Folia Anat Jpn. 2010. 87:49–58.
Article22. Henrich M. Clinical topography of the proctodeum. Acta Anat (Basel). 1980. 106:161–170.
Article23. Courtney H. Anatomy of the pelvic diaphragm and anorectal musculature as related to sphincter preservation in anorectal surgery. Am J Surg. 1950. 79:155–173.
Article24. Arakawa T, Murakami G, Nakajima F, Matsubara A, Ohtsuka A, Goto T, et al. Morphologies of the interfaces between the levator ani muscle and pelvic viscera, with special reference to muscle insertion into the anorectum in elderly Japanese. Anat Sci Int. 2004. 79:72–81.
Article25. Shafik A. New concept of the anatomy of the anal sphincter mechanism and the physiology of defecation. II. Anatomy of the levator ani muscle with special reference to puborectalis. Invest Urol. 1975. 13:175–182.26. Shafik A. Levator ani muscle: new physioanatomical aspects and role in the micturition mechanism. World J Urol. 1999. 17:266–273.
Article27. García-Armengol J, García-Botello S, Martinez-Soriano F, Roig JV, Lledó S. Review of the anatomic concepts in relation to the retrorectal space and endopelvic fascia: waldeyer's fascia and the rectosacral fascia. Colorectal Dis. 2008. 10:298–302.
Article28. McKirdy HC. Anatomy and function of the anal longitudinal muscle. Br J Surg. 1993. 80:262.
Article29. Olson L, Alund M. Quinacrine-binding nerves: presence in the mouse ano-coccygeus muscle, disappearance after muscle transsection. Med Biol. 1979. 57:182–186.30. Hirata E, Koyama M, Murakami G, Ohtsuka A, Abe S, Ide Y, et al. Comparative histological study of levels 1-3 supportive tissues using pelvic floor semiserial sections from elderly nulliparous and multiparous women. J Obstet Gynaecol Res. 2011. 37:13–23.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Perineal raphe with special reference to its extension to the anus: a histological study using human fetuses
- The effect of treatment with tryptophan and/or reserpine on the serotonergic immunoreactivity in raphe nucleus of medulla oblongata and midbrain of the rats
- A temporary disc-like structure at the median atlanto-axial joint in human fetuses
- Distally-extending muscle fibers across involved joints: study of long muscles and tendons of wrist and ankle in late-term fetuses and adult cadavers
- Embryologic Discission of the Median Raphe Cyst: Two Cases Report
