J Korean Med Sci.
2007 Apr;22(2):254-257. 10.3346/jkms.2007.22.2.254.
A Comparative Study of Pericostal and Submuscular Bar Fixation Technique in the Nuss Procedure
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Guro Hospital, Korea University Medical Center, 97 Guro-donggil, Guro-gu, Seoul, Korea. kughcs@korea.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Kangwon National University Hospital, Chuncheon, Korea.
- KMID: 1713180
- DOI: http://doi.org/10.3346/jkms.2007.22.2.254
Abstract
- We evaluated the safety and stability of the less-invasive submuscular bar fixation method in the Nuss procedure. One hundred and thirteen patients undergoing the Nuss procedure were divided into three groups according to the bar fixation technique employed. Group 1 consisted of 25 patients who had undergone bilateral pericostal bar fixation, group 2 consisted of 39 patients with unilateral pericostal one, and group 3 included 49 patients with bilateral submuscular one. The patients' age ranged from 2 to 25 yr, with an average of 7.2+/-5.67 yr. Bar dislocation occurred in 1 patient (4%) in Group 1, 2 patients (5.1%) in Group 2, and 1 patient (2.0%) in Group 3 (p=0.46). Hemothorax was noted in 2 patients (8%) in Group 1, 2 (5.1%) in Group 2, and none (0%) in Group 3 (Group 1 vs. Group 3, p=0.028). The mean operation time was shorter in Group 3 than Group 1 (50.1+/-21.00 in Group 3 vs. 67.2+/-33.07 min in Group 1, p=0.041). The submuscular bar fixation results in a decrease in technique-related complications and operation time and is associated with favorable results with regard to the prevention of bar dislodgement.
MeSH Terms
-
Treatment Outcome
Thoracic Surgical Procedures/*instrumentation/*methods
Surgical Procedures, Minimally Invasive/instrumentation/methods
Ribs/surgery
Reconstructive Surgical Procedures/*instrumentation/*methods
*Prostheses and Implants
Male
Humans
Funnel Chest/*surgery
Female
Child, Preschool
Child
Adult
Adolescent
Abdominal Muscles/surgery
Figure
-
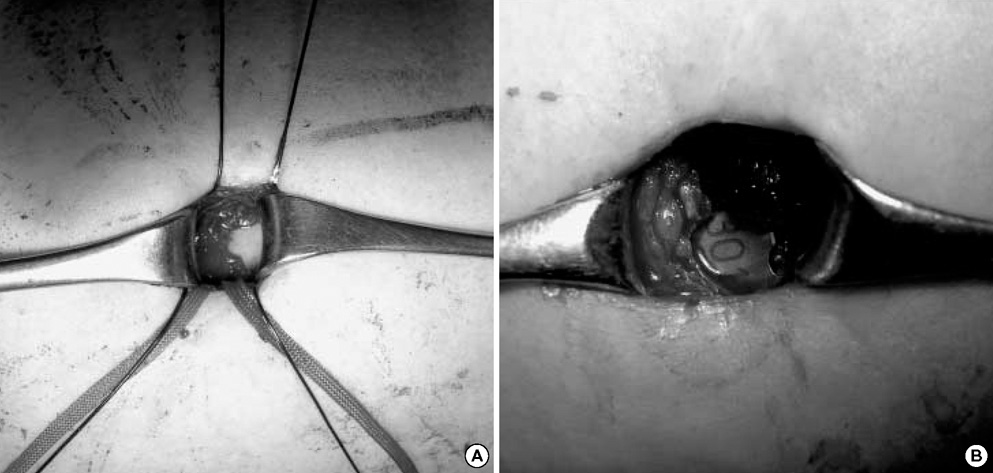
Fig. 1 (A) The serratus anterior muscle is dissected away from the ribs via electrocauterization, then sutured with PDS 1-0 in order to firmly secure the bar. (B) Bar is inserted into the submuscular area.
Reference
-
1. Ravitch MM. Operative treatment of congenital deformities of the chest. Am J Surg. 1961. 101:588–597.
Article2. Nuss D, Kelly RE, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg. 1998. 33:545–552.
Article3. Hebra A, Swoveland B, Egbert M, Tagge EP, Geogeson K, Othersen HB Jr, Nuss D. Outcome analysis of minimally invasive repair of pectus excavatum; Review of 251 cases. J Pediatr Surg. 2000. 35:252–255.
Article4. Watanabe A, Watanabe T, Obama T, Ohsawa H, Mawatari T, Ichimiya Y, Abe T. The use of a lateral stabilizer increases the incidence of wound trouble following the Nuss procedure. Ann Thorac Surg. 2004. 77:296–300.
Article5. Hebra A, Gauderer MW, Tagge EP, Adamson WT, Othersen HB Jr. A simple technique for preventing bar displacement with the Nuss repair of pectus excavatum. J Pediatr Surg. 2001. 36:1266–1268.
Article6. Schaarschmidt K, Kolberg-Shwerdt A, Dimitrov G, Straus J. Submuscular bar, multiple pericostal bar fixation, bilateral thoracoscopy: a modified Nuss repair in adolescents. J Pediatr Surg. 2002. 37:1276–1280.
Article7. Park HJ, Lee SY, Lee CS, Youm W, Lee KR. The Nuss procedure for pectus excavatum: evolution of techniques and early results on 322 patients. Ann Thorac Surg. 2004. 77:289–295.
Article8. Molik KA, Engum S, Rescorla F, West KW, Scherer LR, Grosfeld JL. Pectus excavatum repair: experience with standard and minimally invasive techniques. J Pediatr Surg. 2001. 36:324–328.9. Croitoru DP, Kelly RE, Goretsky MJ Jr, Lawson ML, Swoveland B, Nuss D. Experience and modification update for the minimally invasive Nuss technique for pectus excavatum repair in 303 patients. J Pediatr Surg. 2002. 37:437–445.
Article10. Miller KA, Woods RK, Sharp RJ, Gittes GK, Wade K, Ashcraft KW, Snyder CL, Andrews WM, Murphy JP, Holcomb GW 3rd. Minimally invasive repair of pectus excavatum: a single institution's experience. Surgery. 2001. 130:652–659.
Article11. Park HJ, Lee SY, Lee CS. Complications associated with the Nuss procedure: analysis of risk factors and suggested measures for prevention of complications. J Pediatr Surg. 2004. 39:391–395.
Article12. Jo WM, Choi YH, Sonh YS, Kim HJ, Hwang JJ, Cho SJ. Surgical treatment for pectus excavatum. J Korean Med Sci. 2003. 18:360–364.
Article13. Davis JT, Weinstein S. Repair of the pectus deformity: results of the Ravitch approach in the current era. Ann Thorac Surg. 2004. 78:421–426.
Article14. Fonkalsrud EW. Open repair of pectus excavatum with minimal cartilage resection. Ann Surg. 2004. 240:231–235.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Successful Application of Nuss Procedures with Modified Operative Technique
- Minimally Invasive Repair of Pectus Excavatum Based on the Nuss Principle: An Evolution of Techniques and Early Results on 322 Patients
- Tension Pneumothorax following the Insertion of a Stainless Steel Bar in Patients undergoing the Pectus Excavatum Repair by the Nuss Procedure : A case report
- Embarrassed Radiofrequency Catheter Ablation of Supraventricular Tachycardia in Pectus Excavatum
- Surgical Treatment for Pectus Excavatum
