An Immunoglobulin G4-Related Sclerosing Disease of the Small Bowel: CT and Small Bowel Series Findings
- Affiliations
-
- 1Department of Radiology, Hallym University Dongtan Sacred Heart Hospital, Hwaseong 445-907, Korea.
- 2Department of Radiology, Hallym University Kangnam Sacred Heart Hospital, Seoul 150-950, Korea. baccas@hallym.or.kr
- 3Department of Pathology, Hallym University Kangnam Sacred Heart Hospital, Seoul 150-950, Korea.
- KMID: 1711432
- DOI: http://doi.org/10.3348/kjr.2013.14.5.776
Abstract
- Immunoglobulin G4 (IgG4)-related sclerosing disease is rare and is known to involve various organs. We present a case of histologically proven IgG4-related sclerosing disease of the small bowel with imaging findings on computed tomography (CT) and small bowel series. CT showed irregular wall thickening, loss of mural stratification and aneurysmal dilatation of the distal ileum. Small bowel series showed aneurysmal dilatations, interloop adhesion with traction and abrupt angulation.
MeSH Terms
Figure
-
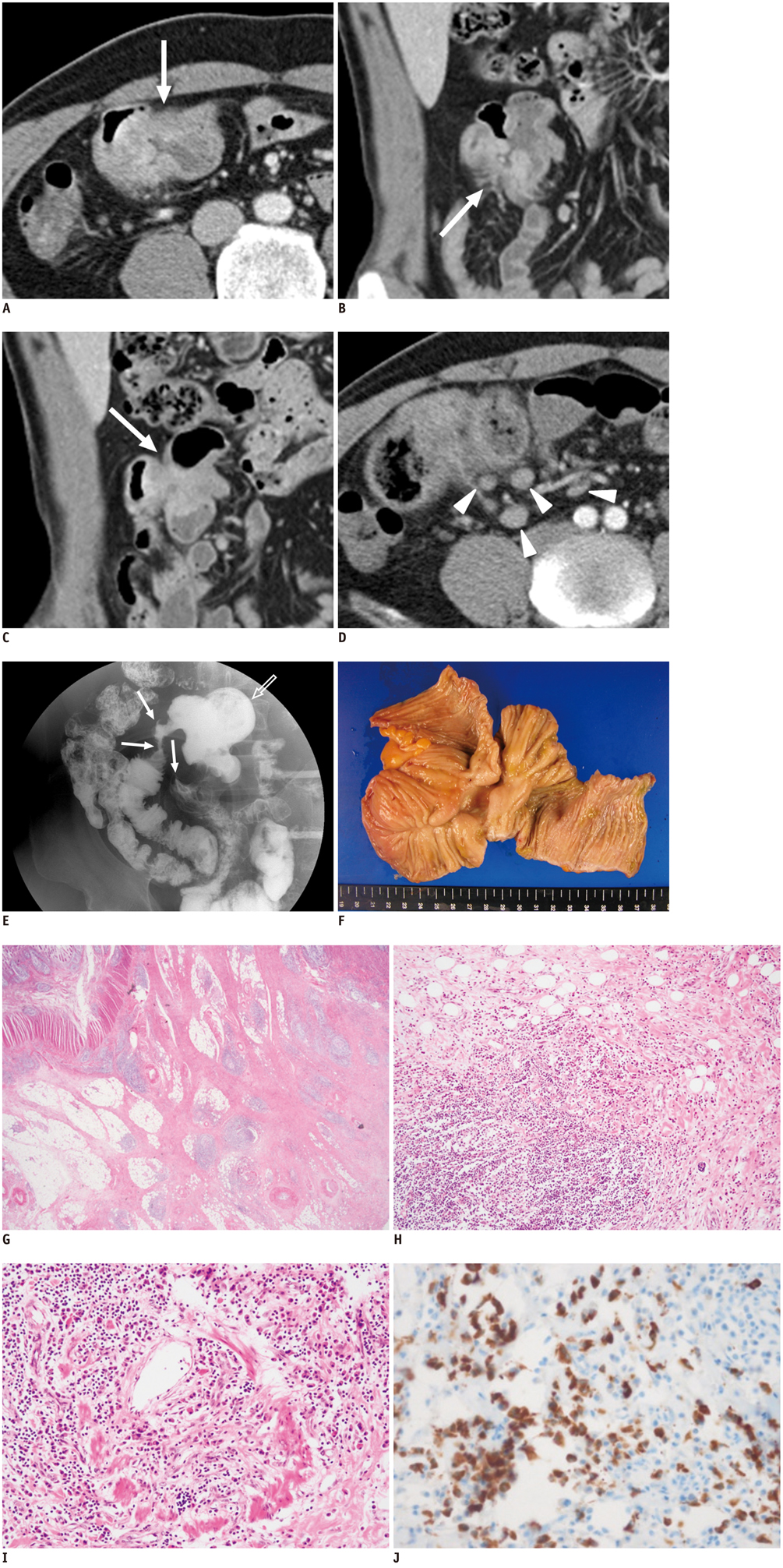
Fig. 1 CT, small bowel series, and histologic findings in 43-year-old man with IgG4-related sclerosing disease of small bowel. Contrast-enhanced axial (A) and coronal-reformatted (B) CT images show irregular thickening, loss of mural stratification and heterogeneous enhancement of distal ileal wall (arrows). Lesion also reveals aneurysmal dilatation. Another coronal-reformatted CT image (C) shows adhesion and aggregation of few small bowel loops (arrow). Another axial CT image (D) reveals multiple enlarged lymph nodes (arrowheads). Small bowel series (E) shows aggregation of distal ileum with traction, angulation and abrupt narrowing which indicates adhesion of ileal loops (arrows). Aneurysmal dilatation of involved segment is also noted (open arrow). On gross specimen (F) obtained from segmental bowel resection, resected ileum shows depressed lesion (4 × 3 cm) with thickened and edematous wall, forming interloop adhesion. On microscopic examination (G-I), ill-demarcated fibrotic lesion involving submucosa, muscle layer and serosa is seen with prominent lymphoplasmacytic infiltrate (G, Hematoxylin & Eosin, × 10). Lymphoplasmacytic infiltrates occasionally show germinal centers (H) and obliterative phlebitis is present (I). Immunohistochemical stain (J) reveals many IgG4-positive plasma cells (more than 50/high power field).
Reference
-
1. Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008; 14:3948–3955.2. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539–551.3. Wong DD, Pillai SR, Kumarasinghe MP, McGettigan B, Thin LW, Segarajasingam DS, et al. IgG4-related sclerosing disease of the small bowel presenting as necrotizing mesenteric arteritis and a solitary jejunal ulcer. Am J Surg Pathol. 2012; 36:929–934.4. Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K, Hayashi N. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci. 1995; 40:1561–1568.5. Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003; 38:982–984.6. Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol. 2010; 34:1812–1819.7. Cheuk W, Chan JK. IgG4-related sclerosing disease: a critical appraisal of an evolving clinicopathologic entity. Adv Anat Pathol. 2010; 17:303–332.8. Yamamoto H, Yamaguchi H, Aishima S, Oda Y, Kohashi K, Oshiro Y, et al. Inflammatory myofibroblastic tumor versus IgG4-related sclerosing disease and inflammatory pseudotumor: a comparative clinicopathologic study. Am J Surg Pathol. 2009; 33:1330–1340.9. Saab ST, Hornick JL, Fletcher CD, Olson SJ, Coffin CM. IgG4 plasma cells in inflammatory myofibroblastic tumor: inflammatory marker or pathogenic link? Mod Pathol. 2011; 24:606–612.10. Kuroiwa T, Suda T, Takahashi T, Hirono H, Natsui M, Motoyama H, et al. Bile duct involvement in a case of autoimmune pancreatitis successfully treated with an oral steroid. Dig Dis Sci. 2002; 47:1810–1816.11. Kamisawa T, Okamoto A. Autoimmune pancreatitis: proposal of IgG4-related sclerosing disease. J Gastroenterol. 2006; 41:613–625.12. Hamano H, Arakura N, Muraki T, Ozaki Y, Kiyosawa K, Kawa S. Prevalence and distribution of extrapancreatic lesions complicating autoimmune pancreatitis. J Gastroenterol. 2006; 41:1197–1205.13. Choi JW, Kim SY, Moon KC, Cho JY, Kim SH. Immunoglobulin G4-related sclerosing disease involving the urethra: case report. Korean J Radiol. 2012; 13:803–807.14. Fukukura Y, Fujiyoshi F, Nakamura F, Hamada H, Nakajo M. Autoimmune pancreatitis associated with idiopathic retroperitoneal fibrosis. AJR Am J Roentgenol. 2003; 181:993–995.15. Zamboni G, Lüttges J, Capelli P, Frulloni L, Cavallini G, Pederzoli P, et al. Histopathological features of diagnostic and clinical relevance in autoimmune pancreatitis: a study on 53 resection specimens and 9 biopsy specimens. Virchows Arch. 2004; 445:552–563.16. Moh IH, Kim JB, Shin SR, Jung SW, Park SH, Kim JW, et al. A case of intraperitoneal immunoglobulin G4-related inflammatory pseudotumor. Korean J Gastroenterol. 2012; 60:258–261.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immunoglobulin G4-related sclerosing cholangitis
- Radiologic Review of Small Bowel Malignancies and Their Mimicking Lesions
- A Case of Immunoglobulin G4-Related Sclerosing Disease Mimicking Lung Cancer
- Primary malignant small bowel tumor
- Immunoglobulin G4-related Disease of the Small Bowel: A Case of Long-term Remission Achieved by Surgical Resection without Maintenance Therapy
