Clinical, Pathological, and Immunohistochemical Features of Adenomyoma in the Ampulla of Vater
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea. smpark@chungbuk.ac.kr
- 2Department of Radiology, Chungbuk National University College of Medicine, Cheongju, Korea.
- 3Department of Pathology, Chungbuk National University College of Medicine, Cheongju, Korea.
- 4Department of Surgery, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 1711291
- DOI: http://doi.org/10.4166/kjg.2013.62.6.352
Abstract
- BACKGROUND/AIMS
Ampullary adenomyoma is a benign lesion whose malignant potential has yet to be confirmed. Despite its benign nature, adenomyoma is frequently misdiagnosed as a carcinoma or adenoma and is overtreated by extensive surgery. This study was performed to analyze the clinical, pathological, and immunohistochemical features of adenomyomas in the ampulla of Vater.
METHODS
Nine cases of adenomyoma in the ampulla of Vater, diagnosed in Chungbuk National University Hospital between 2008 and 2011, were enrolled in this study. We reviewed the clinical data on the symptoms, laboratory data, and radiologic findings of the abdominal computed tomography and endoscopic retrograde cholangiopancreatography. For pathological analysis, all the slides were reviewed by one pathologist, and immunohistochemical stainings with antibodies against cytokeratin 7 (CK7), cytokeratin 20 (CK20), alpha-smooth muscle actin (alpha-SMA), and Ki-67 antigen were performed.
RESULTS
All the cases were CK7 positive and CK20 negative. A strong cytoplasmic expression of alpha-SMA was confirmed in all cases. The Ki-67 index was less than 1% in eight cases and 5% in one case. Four cases underwent endoscopic papillectomy, and one case received surgical ampullectomy during colorectal cancer surgery. Five cases that underwent endoscopic or surgical treatment remained symptom-free for three years. Four cases that were closely observed with repeated endoscopic examinations exhibited no interval changes in the papillary lesions.
CONCLUSIONS
Endoscopic biopsy and immunohistochemistry can aid in the diagnosis of ampullary adenomyomas. Endoscopic papillectomy or surgical ampullectomy is adequate for the treatment of symptomatic ampullary adenomyomas.
Keyword
MeSH Terms
-
Actins/metabolism
Adenomyoma/*pathology/surgery
Aged
Ampulla of Vater/*pathology
Cholangiopancreatography, Endoscopic Retrograde
Common Bile Duct Neoplasms/*pathology/surgery
Female
Humans
Immunohistochemistry
Keratin-20/metabolism
Keratin-7/metabolism
Ki-67 Antigen/metabolism
Male
Middle Aged
Retrospective Studies
Tomography, X-Ray Computed
Treatment Outcome
Actins
Keratin-20
Keratin-7
Ki-67 Antigen
Figure
-

Fig. 1. Radiologic findings of adenomyomas in the ampulla of Vater. Abdominal CT (A, axial view; B, coronal view) showed a 1.4-cm mass protruding into the duodenal lumen with a dilated common bile duct (arrows). (C) Endoscopic retrograde cholangiopancreatography showed a dilated biliary tract (arrow).

Fig. 2. Endoscopic view of ampullary adenomyomas. Enlarged major papilla and villous and granular mucosa around the papillary orifice could be identified in all cases; each case matched from A to I.
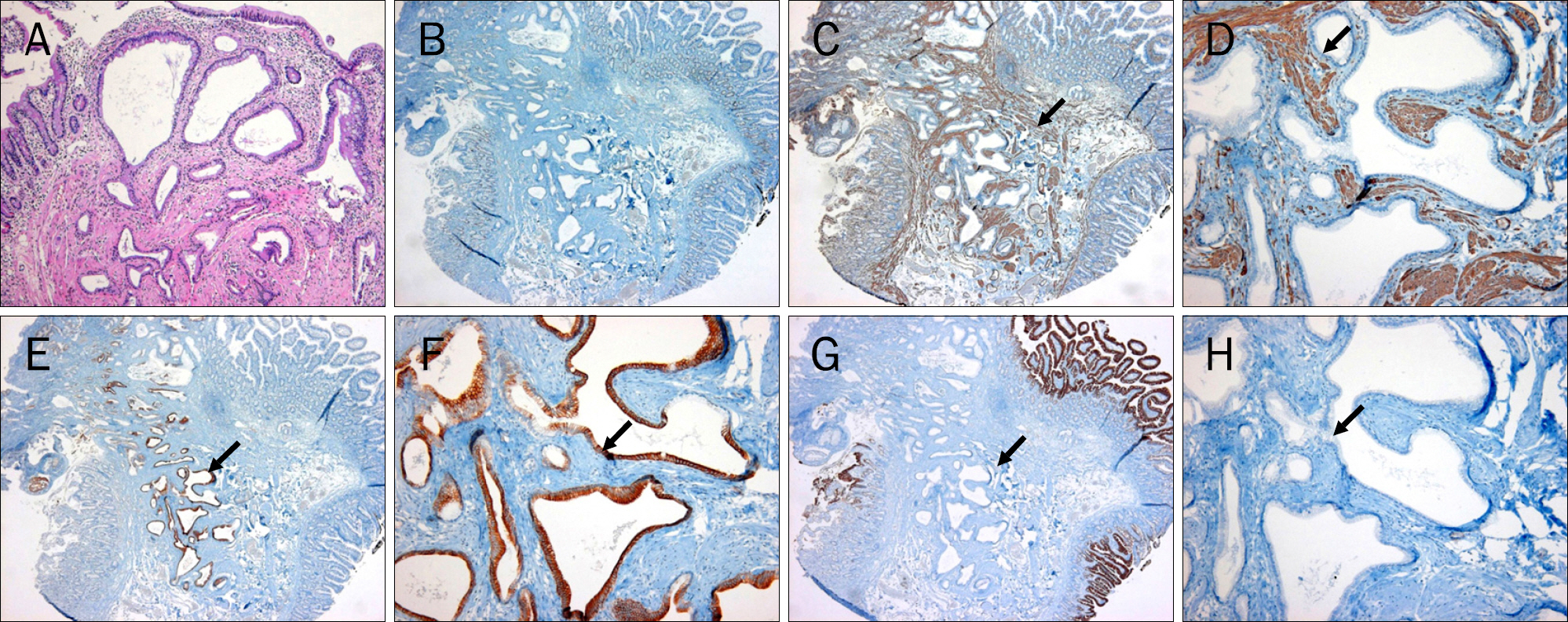
Fig. 3. Pathological and immunohistochemical features of adenomyomas in the ampulla of Vater. (A) Hyperplastic glandular lobules covered by a single layer of epithelium were surrounded by hyperplastic mesenchymal tissues composed of muscle fibers, fibroblasts, myofibroblasts, and capillaries (H&E, ×200). (B) Immunohistochemical staining with the Ki67 antibody level detected at less than 1% (×40). (C, D) α-SMA expression (arrows) in the myofibroblastic component (×40 and ×400, respectively). (E, F) Strong CK7 expression (arrows) in the epithelial lining of the glandular structures (×40 and ×400, respectively). (G, H) No CK20 expression (arrows) in the epithelial lining of the glandular structures (×40 and ×400, respectively).
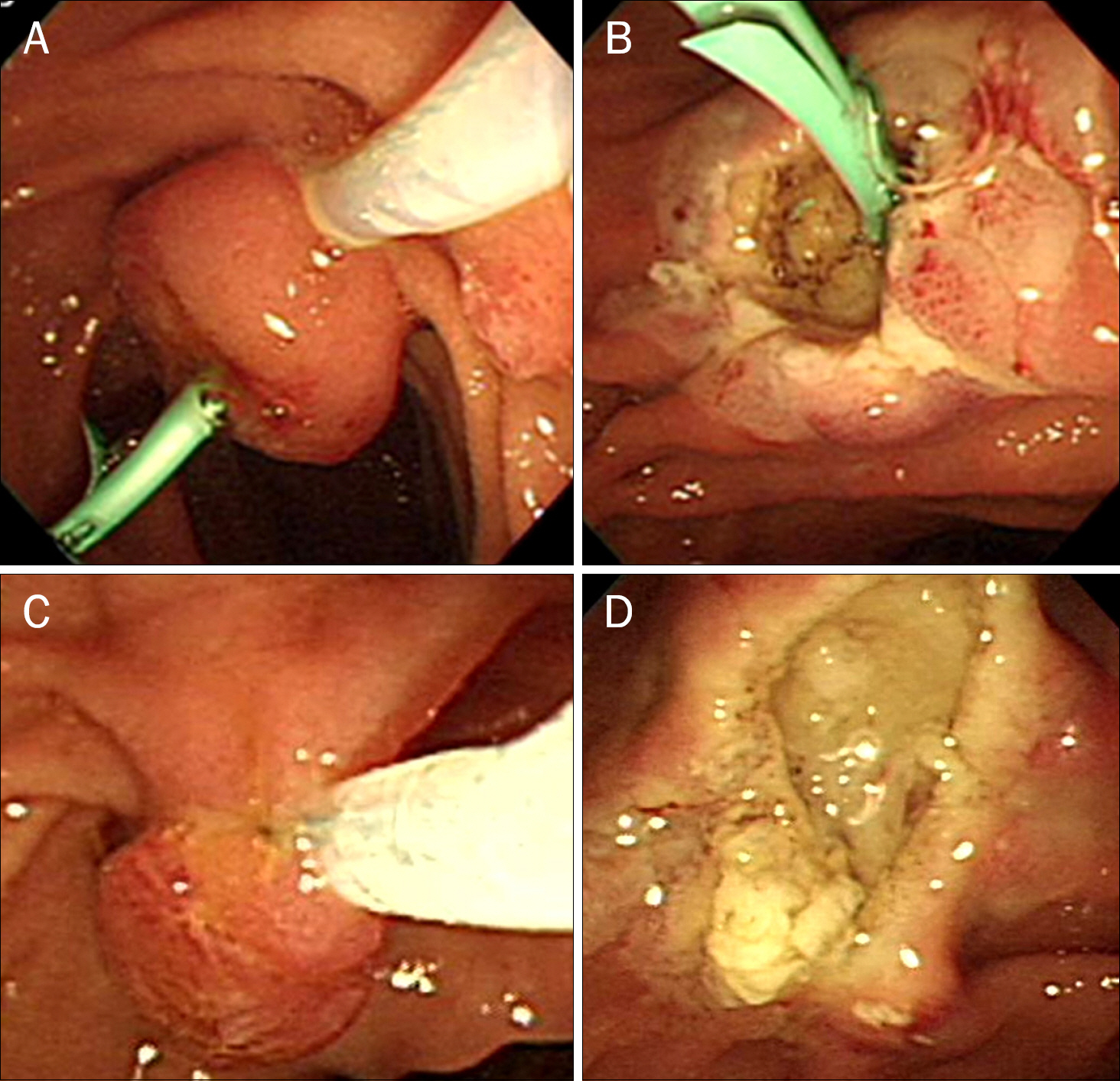
Fig. 4. Endoscopic papillectomy for an ampullary adenomyoma. (A) Endoscopic papillectomy was performed after pancreatic stent insertion. (B) Endoscopic view of the stent placed in the biliary duct after papillectomy. (C) Endoscopic papillectomy was performed without prior pancreatic stent insertion. (D) Endoscopic view of the major papilla after papillectomy.
Cited by 1 articles
-
Diagnostic Accuracy of the Initial Endoscopy for Ampullary Tumors
Hee Seung Lee, Jong Soon Jang, Seungho Lee, Myeong Ho Yeon, Ki Bae Kim, Jae Geun Park, Joo Young Lee, Mi Jin Kim, Joung-Ho Han, Rohyun Sung, Seon Mee Park
Clin Endosc. 2015;48(3):239-246. doi: 10.5946/ce.2015.48.3.239.
Reference
-
References
1. Handra-Luca A, Terris B, Couvelard A, Bonte H, Flejou JF. Adenomyoma and adenomyomatous hyperplasia of the Vaterian system: clinical, pathological, and new immunohistochemical features of 13 cases. Mod Pathol. 2003; 16:530–536.
Article2. Albores-Saavedra JH, Sobin LH, Gibson JB. Histological typing of tumours of the gallbladder and extrahepatic bile ducts. Berlin: Springer-Verlag;1991.3. Hammarström LE, Holmin T, Stenram U. Adenomyoma of the ampulla of Vater: an uncommon cause of bile duct obstruction. Surg Laparosc Endosc. 1997; 7:388–393.4. Narita T, Yokoyama M. Adenomyomatous hyperplasia of the papilla of Vater: A sequela of chronic papillitis? Ann Diagn Pathol. 1999; 3:174–177.
Article5. Clarke BE. Myoepithelial hamartoma of the gastrointestinal tract. Arch Pathol. 1940; 30:143–152.6. Fernandez-Cruz L, Pera C. A histological study of the sphincter of Oddi. In: Delmont J, ed. The sphincter of Oddi. Proceedings of the 3rd Gastroenterology Symposium. Nice: Gastroenterology Symposium. 1976. 13–20.7. Kim JW, Jang JY, Han SS, Choi MK, Kim SH, Park YH. Adenomyoma of the Vaterian ampulla. Korean J Hepatobiliary Pancreat Surg. 2004; 8:258–261.8. Jang KT, Heo JS, Choi SH, et al. Adenomyoma of ampulla of Vater or the common bile duct: a report of three cases. Korean J Pathol. 2005; 39:59–62.9. Kwon TH, Park do H, Shim KY, et al. Ampullary adenomyoma presenting as acute recurrent pancreatitis. World J Gastroenterol. 2007; 13:2892–2894.
Article10. Lee BU, Bang JS, Yang SH, et al. A case of ampullary adenomyoma associated with dilatations of pancreatic and biliary ducts. Korean J Gastrointest Endosc. 2010; 40:391–395.11. Menzel J, Poremba C, Dietl KH, Böcker W, Domschke W. Tumors of the papilla of Vater–inadequate diagnostic impact of endoscopic forceps biopsies taken prior to and following sphincterotomy. Ann Oncol. 1999; 10:1227–1231.12. Bedirli A, Patiroglu TE, Sozuer EM, Sakrak O. Periampullary adenomyoma: report of two cases. Surg Today. 2002; 32:1016–1018.13. Kayahara M, Ohta T, Kitagawa H, Miwa K, Urabe T, Murata T. Adenomyomatosis of the papilla of Vater: a case illustrating diagnostic difficulties. Dig Surg. 2001; 18:139–142.
Article14. Läuffer JM, Baer HU, Maurer CA, et al. Adenomyoma of the distal common bile duct mimicking cholangiocarcinoma. Dig Dis Sci. 1998; 43:1200–1204.15. Higashi M, Goto M, Saitou M, et al. Immunohistochemical study of mucin expression in periampullary adenomyoma. J Hepatobiliary Pancreat Sci. 2010; 17:275–283.
Article16. Duval JV, Savas L, Banner BF. Expression of cytokeratins 7 and 20 in carcinomas of the extrahepatic biliary tract, pancreas, and gallbladder. Arch Pathol Lab Med. 2000; 124:1196–1200.
Article17. Sheehan M, O'Briain DS. False-positive immunoreactivity with muscle-specific actins in non-Hodgkin's lymphomas. Arch Pathol Lab Med. 1995; 119:225–228.18. Scholzen T, Gerdes J. The Ki-67 protein: from the known and the unknown. J Cell Physiol. 2000; 182:311–322.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenomyoma of the Vaterian Ampulla
- A Case of Ampullary Adenomyoma Associated with Dilatations of Pancreatic and Biliary Ducts
- Adenomyoma of Ampulla of Vater or the Common Bile Duct: A Report of Three Cases
- Ampulla of Vater Adenomyoma with Dilatations of Biliary and Pancreatic Duct
- Differentiation of Adenomyoma from Localized Adenocarcinoma of the Ampulla of Vater Using Multidetector CT
