Korean J Gastroenterol.
2013 Jul;62(1):55-58. 10.4166/kjg.2013.62.1.55.
A Case of Isolated Small Intestinal Wall Calcification on Patient with Continuous Ambulatory Peritoneal Dialysis
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea. hands@hanyang.ac.kr
- KMID: 1711280
- DOI: http://doi.org/10.4166/kjg.2013.62.1.55
Abstract
- The metastatic calcification is defined as the deposition of calcium salt in normal tissue with an abnormal serum biochemical environment, such as chronic kidney disease, hyperparathyroidism, and hypercalcemia related with malignancy. Although the metastatic calcification can develop in any organs and tissues, presenting its symptoms and complications are rare. Thus a few cases have been reported. This case shows the metastatic calcification of the small intestine without any peritoneal and mesenteric vascular calcification which was early diagnosed by computed tomography and mesenteric angiography in a patient with abdominal pain, receiving continuous ambulatory peritoneal dialysis due to end stage renal disease. The clinician should early consider the metastatic calcification as differential diagnosis when unidentified calcifications are noted in simple abdominal X-ray such as in the present case, and promptly confirm it by using appropriate diagnostic tests in order to prevent its complications and progression.
MeSH Terms
-
Calcinosis/*diagnosis/drug therapy/etiology
Calcitriol/therapeutic use
Calcium/blood
Calcium Carbonate/therapeutic use
Calcium Channel Agonists/therapeutic use
Humans
Intestine, Small/*radiography
Kidney Failure, Chronic/therapy
Male
Mesenteric Artery, Superior/radiography
Middle Aged
Peritoneal Dialysis, Continuous Ambulatory/*adverse effects
Tomography, X-Ray Computed
Calcitriol
Calcium
Calcium Carbonate
Calcium Channel Agonists
Figure
-
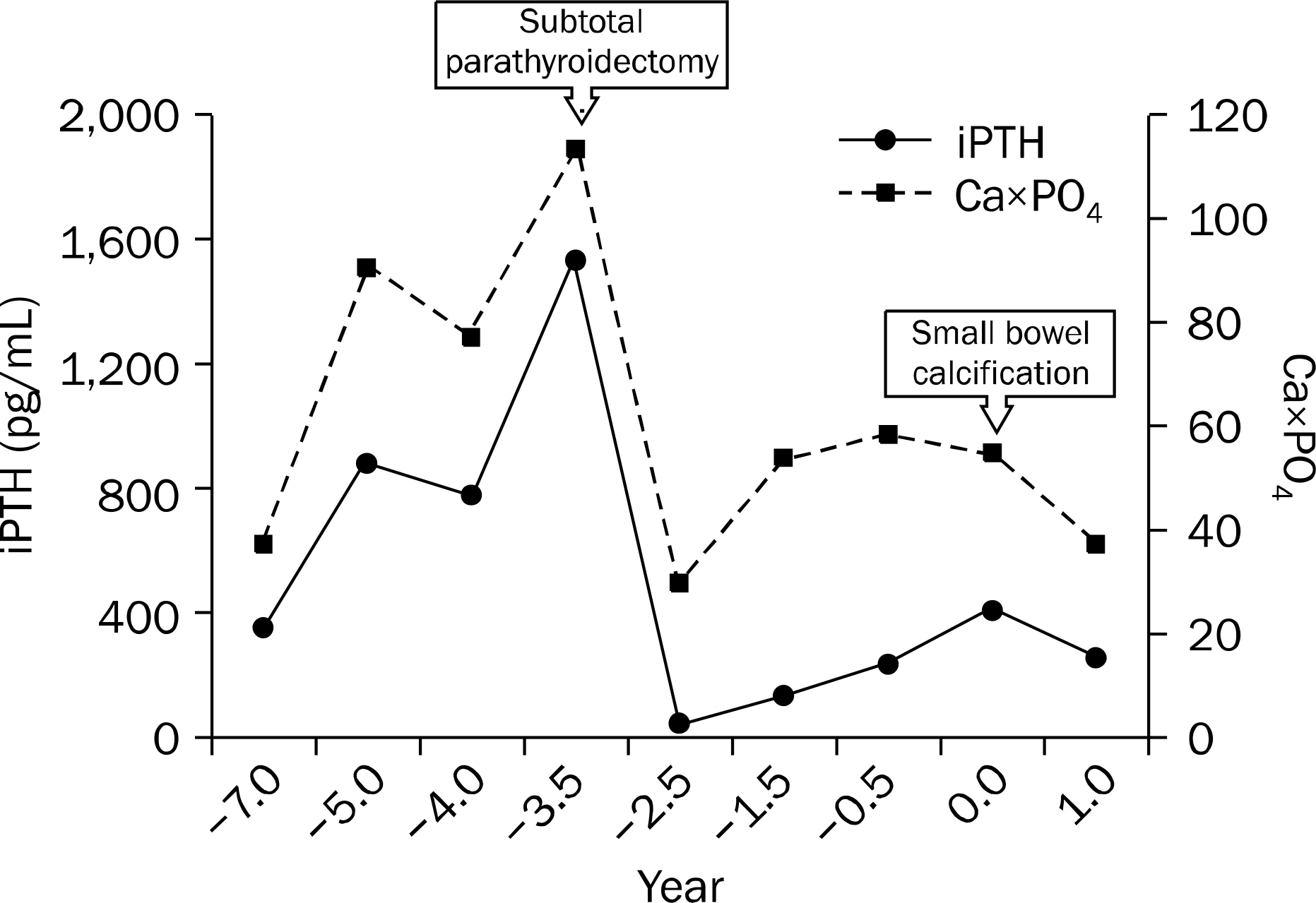
Fig. 1. The changes of intact parathyroid hormone (iPTH) level and calcium-phosphorous product (Ca×PO4).
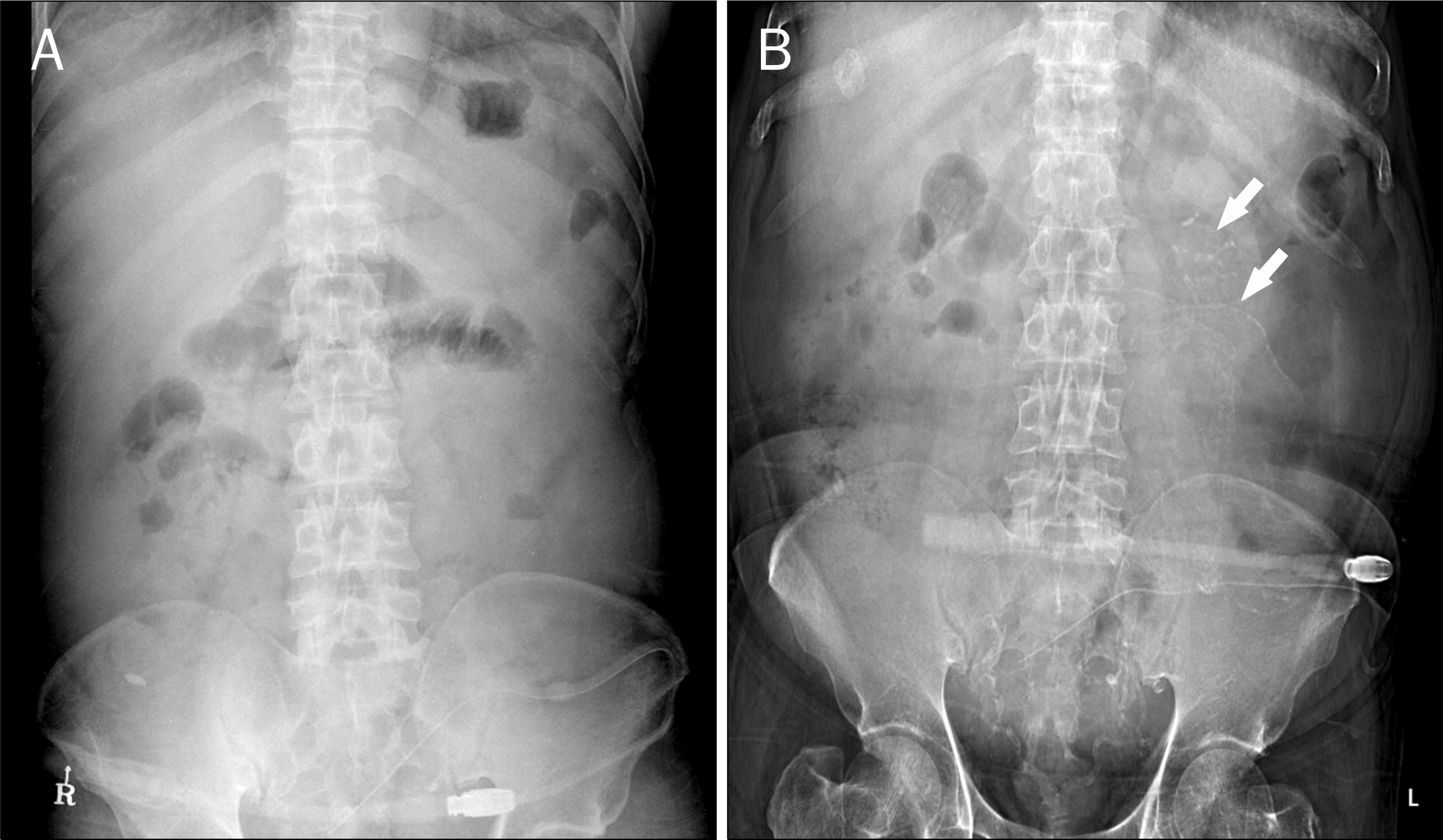
Fig. 2. Plain abdominal X-ray showed calcification (arrows) in the left upper quadrant (B) although it had not shown in previous plain X-ray (A).
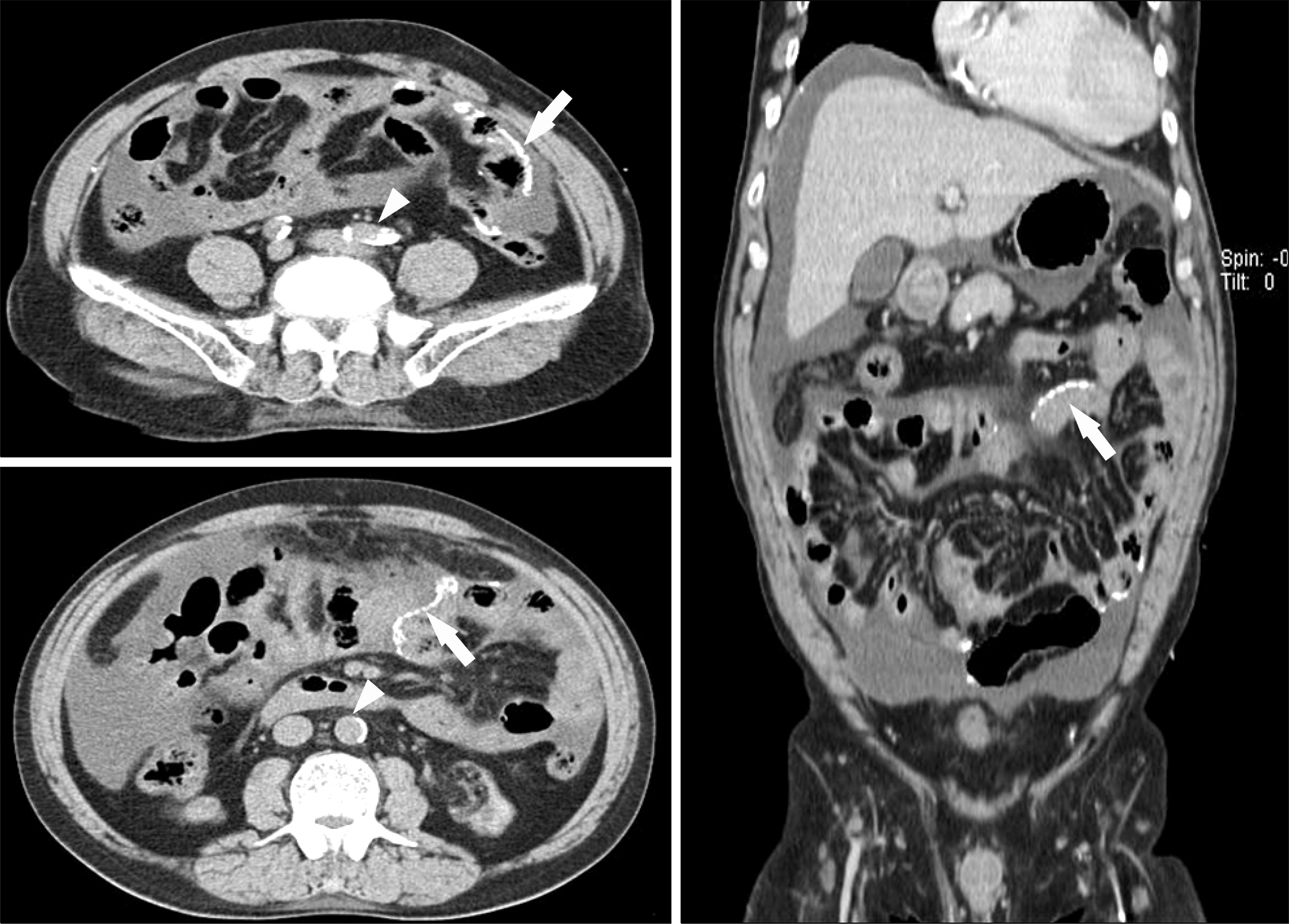
Fig. 3. Abdominal CT scan showed linear calcification along jejunal wall (arrows). Also, aortic calcification was also noted (arrowheads).
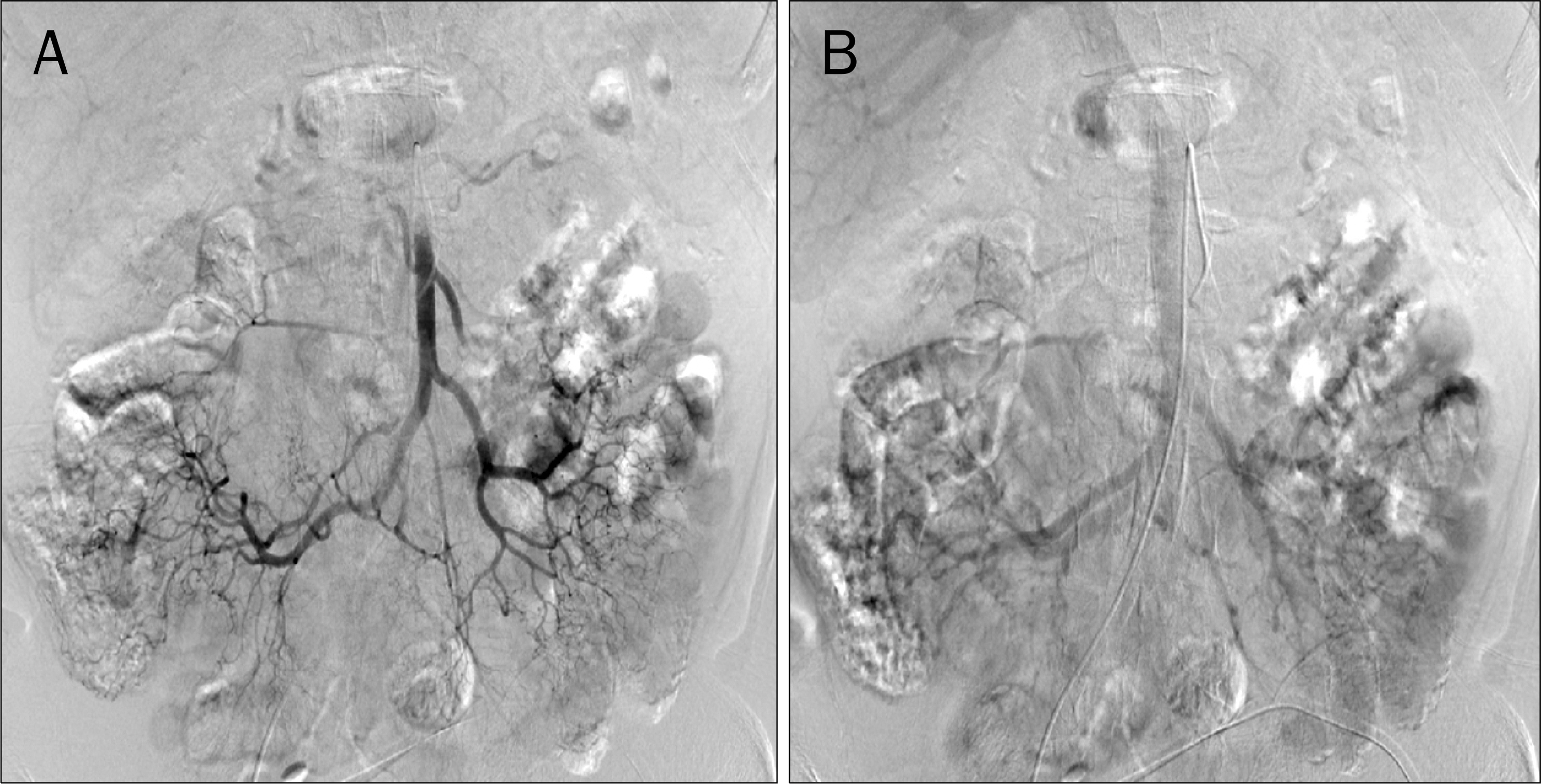
Fig. 4. Superior mesenteric artery angiography of arterial phase (A) and portal phase (B). There were no abnormal findings on both arteries and veins. Mural calcification on small bowel was noted.
Reference
-
References
1. Ketteler M, Rothe H, Krüger T, Biggar PH, Schlieper G. Mechanisms and treatment of extraosseous calcification in chronic kidney disease. Nat Rev Nephrol. 2011; 7:509–516.
Article2. Block GA, Hulbert-Shearon TE, Levin NW, Port FK. Association of serum phosphorus and calcium × phosphate product with mortality risk in chronic hemodialysis patients: a national study. Am J Kidney Dis. 1998; 31:607–617.3. Salem MM. Hyperparathyroidism in the hemodialysis population: a survey of 612 patients. Am J Kidney Dis. 1997; 29:862–865.
Article4. Li YJ, Tian YC, Chen YC, et al. Fulminant pulmonary calciphylaxis and metastatic calcification causing acute respiratory failure in a uremic patient. Am J Kidney Dis. 2006; 47:e47–e53.
Article5. Cha I, Cho E, Yoon K, et al. A case of peritonitis induced by small bowel calcification and microperforation: sustained secondary hyperparathyroidism in a patient with continuous peritoneal dialysis. Korean J Nephrol. 2010; 29:529–534.6. Alfrey AC. The role of abnormal phosphorus metabolism in the progression of chronic kidney disease and metastatic calcification. Kidney Int Suppl. 2004; (90):S13–S17.
Article7. Gorospe M, Fadare O. Gastric mucosal calcinosis: clinicopathologic considerations. Adv Anat Pathol. 2007; 14:224–228.8. Moe SM, Duan D, Doehle BP, O'Neill KD, Chen NX. Uremia induces the osteoblast differentiation factor Cbfa1 in human blood vessels. Kidney Int. 2003; 63:1003–1011.
Article9. Cozzolino M, Mazzaferro S, Pugliese F, Brancaccio D. Vascular calcification and uremia: what do we know? Am J Nephrol. 2008; 28:339–346.
Article10. Chen NX, Duan D, O'Neill KD, Moe SM. High glucose increases the expression of Cbfa1 and BMP-2 and enhances the calcification of vascular smooth muscle cells. Nephrol Dial Transplant. 2006; 21:3435–3442.
Article11. Ubara Y, Katori H, Tagami T, et al. Severe ectopic calcification of the intestinal wall in a patient on long-term continuous ambulatory peritoneal dialysis therapy. Am J Kidney Dis. 2000; 35:761–766.
Article12. Poultsidi A, Liakopoulos V, Eleftheriadis T, Zarogiannis S, Bouchlariotou S, Stefanidis I. Gross calcification of the small bowel in a continuous ambulatory peritoneal dialysis patient with sclerosing peritonitis. Adv Perit Dial. 2006; 22:104–107.13. Morris-Stiff GJ, Bowrey DJ, Balaji V, Jurewicz WA. Calcification of the small bowel in renal hyperparathyroidism. J R Soc Med. 1998; 91:430–431.
Article14. Kawanishi H, Kawaguchi Y, Fukui H, et al. Encapsulating peritoneal sclerosis in Japan: a prospective, controlled, multicenter study. Am J Kidney Dis. 2004; 44:729–737.
Article15. Kawaguchi Y, Kawanishi H, Mujais S, Topley N, Oreopoulos DG. Encapsulating peritoneal sclerosis: definition, etiology, diagnosis, and treatment. International Society for Peritoneal Dialysis Ad Hoc Committee on Ultrafiltration Management in Peritoneal Dialysis. Perit Dial Int. 2000; 20(Suppl 4):S43–S55.16. Song JH, Kim JI, Jung JH, et al. A case of phlebosclerotic colitis in a hemodialysis patient. Korean J Gastroenterol. 2012; 59:40–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extensive Peritoneal Calcifications Associated with Continuous Ambulatory Peritoneal Dialysis
- Sclerosing Peritonitis with Gross Calcification: Case Report
- Peritoneal-pleural leak improved by switching from continuous ambulatory peritoneal dialysis to automated peritoneal dialysis
- Incarcerated umbilical hernia with small bowel obstruction in a continuous ambulatory peritoneal dialysis patient
- Persistent Genital Swelling after Hydrocele Ligation in a Patient Receiving Continuous Ambulatory Peritoneal Dialysis
