Acute Central Retinal Artery Occlusion Associated with Livedoid Vasculopathy: A Variant of Sneddon's Syndrome
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. sejoon1@hanmail.net
- 2Department of Biomedical Sciences, Seoul National University Graduate School, Seoul, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 4Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 5Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- KMID: 1707293
- DOI: http://doi.org/10.3341/kjo.2013.27.5.376
Abstract
- Livedoid vasculopathy (LV) is characterized by a long history of ulceration of the feet and legs and histopathology indicating a thrombotic process. We report a case of acute central retinal artery occlusion in a 32-year-old woman who had LV. She showed no discernible laboratory abnormalities such as antiphospholipid antibodies and no history of cerebrovascular accidents. Attempted intra-arterial thrombolysis showed no effect in restoring retinal arterial perfusion or vision. The central retinal artery occlusion accompanied by LV in this case could be regarded as a variant form of Sneddon's syndrome, which is characterized by livedo reticularis and cerebrovascular accidents.
Keyword
MeSH Terms
Figure
-
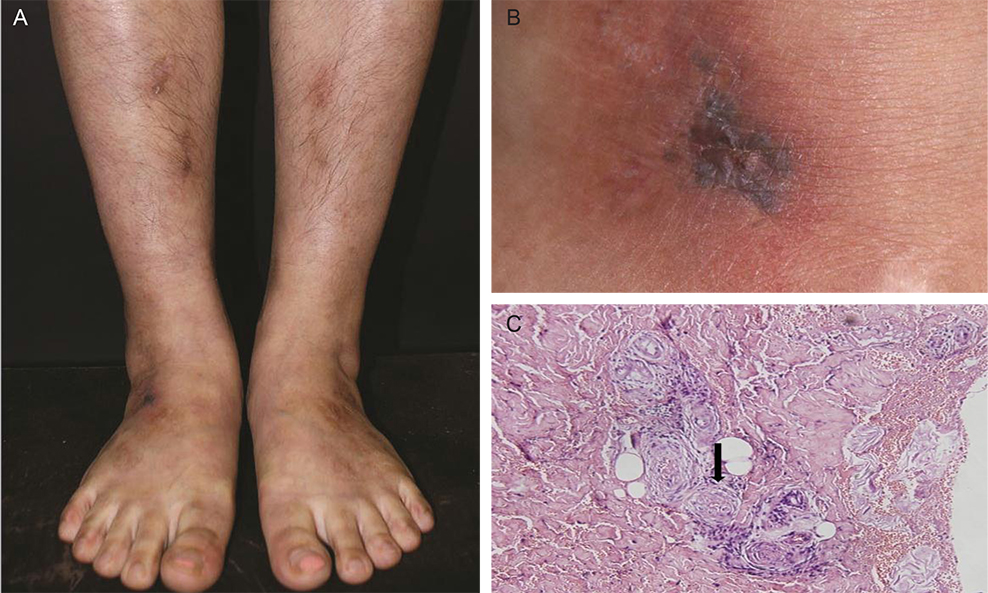
Fig. 1 (A,B) Physical examination of the patient showed itching and tender violaceous to dark erythematous non-elevated patches with central necrotic vesicles on the dorsum of both lower legs and feet. (C) The histopathology of the skin lesion showed perivascular lymphohistiocytic infiltration in the dermis. Fibrin material was observed in the vessel lumen (arrow) and extravasated red blood cells were present. No leukocytoclasis observed (H&E, ×100).

Fig. 2 Fundus photography and fundus fluorescein angiography (FFA) immediately after (A,B) and six weeks after (C,D) intra-arterial thrombolysis (IAT) therapy for acute central retinal artery occlusion. (A) The immediate post-IAT fundus photograph showed no change from the pre-IAT fundus photograph. (B) Early phase FFA still showed delayed retinal arterial filling and arteriovenous transit time. (C) Six weeks after thrombolysis, fundus photography showed severe atrophy of the macula and disc pallor. (D) The retinal arterial perfusion was restored except for the macular area on FFA.
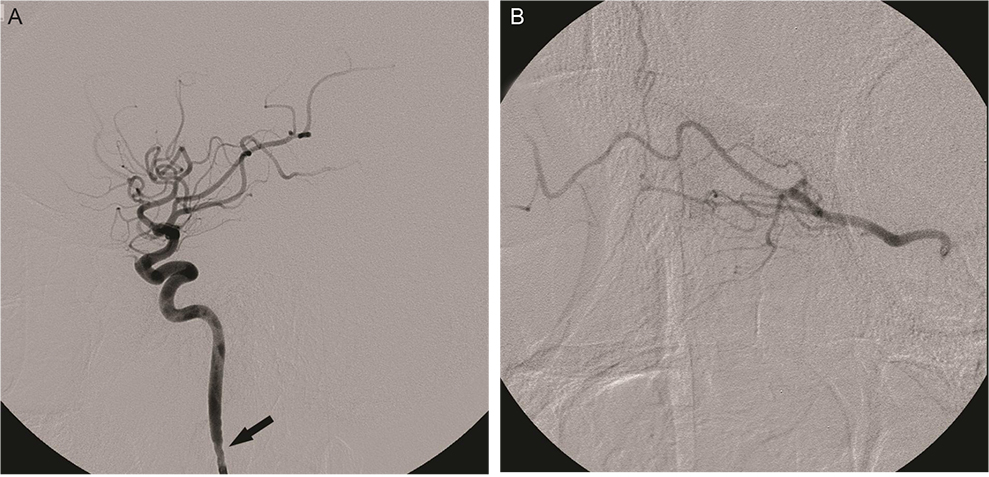
Fig. 3 Right internal carotid angiography before the intra-arterial thrombolysis procedure. (A) Severe vasospasm (arrow) in the proximal cervical internal carotid artery was noted in response to catheter placement, which was relieved by intra-arterial nimodipine infusion (5 mg). (B) Selective angiography of the right ophthalmic artery showed no thrombus or steno-occlusive lesion in the ophthalmic artery.
Reference
-
1. Khenifer S, Thomas L, Balme B, Dalle S. Livedoid vasculopathy: thrombotic or inflammatory disease? Clin Exp Dermatol. 2010; 35:693–698.2. Read RW, Chong LP, Rao NA. Occlusive retinal vasculitis associated with systemic lupus erythematosus. Arch Ophthalmol. 2000; 118:588–589.3. Mirza S, Raghu Ram AR, Bowling BS, Nessim M. Central retinal artery occlusion and bilateral choroidal infarcts in Wegener's granulomatosis. Eye (Lond). 1999; 13(Pt 3a):374–376.4. Warrasak S, Tapaneya-Olarn W, Euswas A, et al. Fibromuscular dysplasia: a rare cause of cilioretinal artery occlusion in childhood. Ophthalmology. 2000; 107:737–741.5. Shimizu K, Numaga J, Takahashi M, Matsunaga T. A case of Sneddon syndrome. Nihon Ganka Gakkai Zasshi. 1995; 99:104–108.6. Jonas J, Kolble K, Volcker HE, Kalden JR. Central retinal artery occlusion in Sneddon's disease associated with antiphospholipid antibodies. Am J Ophthalmol. 1986; 102:37–40.7. Pauranik A, Parwani S, Jain S. Simultaneous bilateral central retinal arterial occlusion in a patient with Sneddon syndrome: case history. Angiology. 1987; 38(2 Pt 1):158–163.8. Alegre VA, Winkelmann RK, Gastineau DA. Cutaneous thrombosis, cerebrovascular thrombosis, and lupus anticoagulant--the Sneddon syndrome: report of 10 cases. Int J Dermatol. 1990; 29:45–49.9. Rehany U, Kassif Y, Rumelt S. Sneddon's syndrome: neuro-ophthalmologic manifestations in a possible autosomal recessive pattern. Neurology. 1998; 51:1185–1187.10. Hayreh SS, Podhajsky PA, Zimmerman MB. Retinal artery occlusion: associated systemic and ophthalmic abnormalities. Ophthalmology. 2009; 116:1928–1936.11. Ivanisević M, Karelovic D. The incidence of central retinal artery occlusion in the district of Split, Croatia. Ophthalmologica. 2001; 215:245–246.12. Kollarits CR, Lubow M, Hissong SL. Retinal strokes. I. Incidence of carotid atheromata. JAMA. 1972; 222:1273–1275.13. Brown GC, Magargal LE, Shields JA, et al. Retinal arterial obstruction in children and young adults. Ophthalmology. 1981; 88:18–25.14. Greven CM, Slusher MM, Weaver RG. Retinal arterial occlusions in young adults. Am J Ophthalmol. 1995; 120:776–783.15. Calamia KT, Balabanova M, Perniciaro C, Walsh JS. Livedo (livedoid) vasculitis and the factor V Leiden mutation: additional evidence for abnormal coagulation. J Am Acad Dermatol. 2002; 46:133–137.16. McCalmont CS, McCalmont TH, Jorizzo JL, et al. Livedo vasculitis: vasculitis or thrombotic vasculopathy? Clin Exp Dermatol. 1992; 17:4–8.17. Klein KL, Pittelkow MR. Tissue plasminogen activator for treatment of livedoid vasculitis. Mayo Clin Proc. 1992; 67:923–933.18. Acland KM, Darvay A, Wakelin SH, Russell-Jones R. Livedoid vasculitis: a manifestation of the antiphospholipid syndrome? Br J Dermatol. 1999; 140:131–135.19. Grob JJ, Bonerandi JJ. Thrombotic skin disease as a marker of the anticardiolipin syndrome: livedo vasculitis and distal gangrene associated with abnormal serum antiphospholipid activity. J Am Acad Dermatol. 1989; 20:1063–1069.20. Biousse V, Calvetti O, Bruce BB, Newman NJ. Thrombolysis for central retinal artery occlusion. J Neuroophthalmol. 2007; 27:215–230.21. Sneddon IB. Cerebro-vascular lesions and livedo reticularis. Br J Dermatol. 1965; 77:180–185.22. Aladdin Y, Hamadeh M, Butcher K. The Sneddon syndrome. Arch Neurol. 2008; 65:834–835.23. Asherson RA, Cervera R, de Groot PG, et al. Catastrophic antiphospholipid syndrome: international consensus statement on classification criteria and treatment guidelines. Lupus. 2003; 12:530–534.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Letter to the Editor: Sneddon's Syndrome versus Susac Syndrome
- Incomplete Central Retinal Artery Occlusion
- A Case of Secondary Antiphospholipid Syndrome with Systemic Erythematosus Lupus Who Presenting Livedo Reticularis, Livedoid Vasculopathy, Peripheral Gangrene, and Leg Ulcers
- The Successful Treatment of a Case of Central Retinal Artery Occlusion
- Central Retinal Artery Occlusion Masquerading as Branch Retinal Artery Occlusion
