Lumbosacral Fixation Using the Diagonal S2 Screw for Long Fusion in Degenerative Lumbar Deformity: Technical Note Involving 13 Cases
- Affiliations
-
- 1Department of Orthopaedic Surgery, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea. hyparkys@hanyang.ac.kr
- KMID: 1705549
- DOI: http://doi.org/10.4055/cios.2013.5.3.225
Abstract
- Placing instrumentation into the ilium has been shown to increase the biomechanical stability and the fusion rates, but it has some disadvantages. The diagonal S2 screw technique is an attractive surgical procedure for degenerative lumbar deformity. Between 2008 and 2010, we carried out long fusion across the lumbosacral junction in 13 patients with a degenerative lumbar deformity using the diagonal S2 screws. In 12 of these 13 patients, the lumbosacral fusion was graded as solid fusion with obvious bridging bone (92%). One patient had a rod dislodge at one S2 screw and breakage of one S1 screw and underwent revision nine months postoperatively. So, we present alternative method of lumbopelvic fixation for long fusion in degenerative lumbar deformity using diagonal S2 screw instead of iliac screw.
MeSH Terms
Figure
-

Fig. 1 Entry point of the S2 alar screw (arrow) and the midpoint of the line from the medial margin of the S1 dorsal foramen and the medial margin of the S2 dorsal foramen.
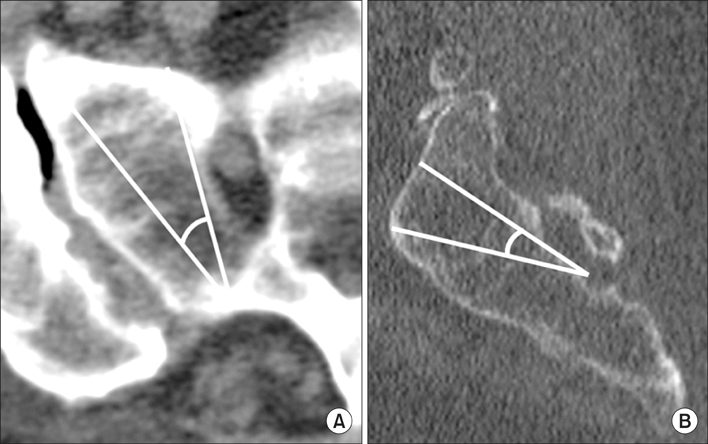
Fig. 2 (A) The lateral trajectory of the S2 alar screw varied somewhat among patients but was typically between 30 and 35 degrees in the lateral planes. It did not penetrate the sacroiliac joint laterally or the S1 ventral foramen medially. (B) The superior trajectory of the S2 alar screw was a longer screw insertion and did vary somewhat among patients, but was typically between 15 and 20 degrees in the superior planes. It did not penetrate the anterior cortex as this could cause impingement of the L5 nerve root and injury to the internal iliac vessels.
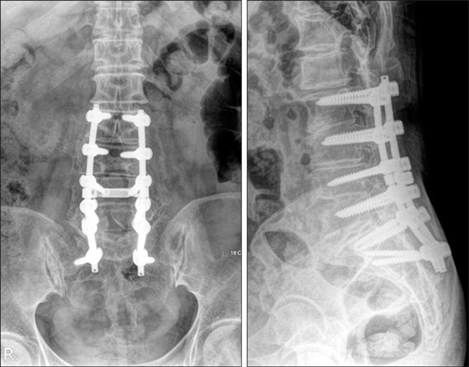
Fig. 3 Two years postoperatively, there was no evidence of screw loosening or pseudarthrosis at the lumbosacral junction.
Reference
-
1. Kuklo TR, Bridwell KH, Lewis SJ, et al. Minimum 2-year analysis of sacropelvic fixation and L5-S1 fusion using S1 and iliac screws. Spine (Phila Pa 1976). 2001; 26(18):1976–1983.
Article2. McCord DH, Cunningham BW, Shono Y, Myers JJ, McAfee PC. Biomechanical analysis of lumbosacral fixation. Spine (Phila Pa 1976). 1992; 17:8 Suppl. S235–S243.
Article3. Lebwohl NH, Cunningham BW, Dmitriev A, et al. Biomechanical comparison of lumbosacral fixation techniques in a calf spine model. Spine (Phila Pa 1976). 2002; 27(21):2312–2320.
Article4. Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine (Phila Pa 1976). 2006; 31(3):303–308.
Article5. Ahn DK, Park HS, Choi DJ, Kim KS, Yang SJ. Survival and prognostic analysis of adjacent segments after spinal fusion. Clin Orthop Surg. 2010; 2(3):140–147.
Article6. Edwards CC 2nd, Bridwell KH, Patel A, Rinella AS, Berra A, Lenke LG. Long adult deformity fusions to L5 and the sacrum: a matched cohort analysis. Spine (Phila Pa 1976). 2004; 29(18):1996–2005.
Article7. Kim YJ, Bridwell KH, Lenke LG, Cho KJ, Edwards CC 2nd, Rinella AS. Pseudarthrosis in adult spinal deformity following multisegmental instrumentation and arthrodesis. J Bone Joint Surg Am. 2006; 88(4):721–728.
Article8. Moshirfar A, Rand FF, Sponseller PD, et al. Pelvic fixation in spine surgery: historical overview, indications, biomechanical relevance, and current techniques. J Bone Joint Surg Am. 2005; 87:Suppl 2. 89–106.9. Leong JC, Lu WW, Zheng Y, Zhu Q, Zhong S. Comparison of the strengths of lumbosacral fixation achieved with techniques using one and two triangulated sacral screws. Spine (Phila Pa 1976). 1998; 23(21):2289–2294.
Article10. Zindrick MR, Wiltse LL, Widell EH, et al. A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop Relat Res. 1986; (203):99–112.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Is S1 Alar Iliac Screw a Feasible Option for Lumbosacral Fixation?: A Technical Note
- Long Segment Fusion to L5 Vertebra and Sacral Vertebra in Degenerative Lumbar Spine
- A Comparison of Clinical Stability of Distal Instrument Fused Down to S1 with and without Sub-S1 Alar Screw in the Long Fusion using Segmental Pedicle Screw for Lumbar Degenerative Deformity
- A Clinical Analysis of Long Segment Fusion with Pedicle Screw in Degenerative Lumbar Spine
- Risk Factors for Loosening of S2 Alar Iliac Screw: Surgical Outcomes of Adult Spinal Deformity
