The Classification of Idiopathic Scoliosis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. choonki@snu.ac.kr
- KMID: 1527144
- DOI: http://doi.org/10.4184/jkss.2007.14.1.57
Abstract
- There are many classifications for idiopathic scoliosis but none of these is perfect. In the treatment of idiopathic scoliosis, it is essential to understand the characteristics of each classification system and exploit their individual advantages.
Keyword
MeSH Terms
Figure
-
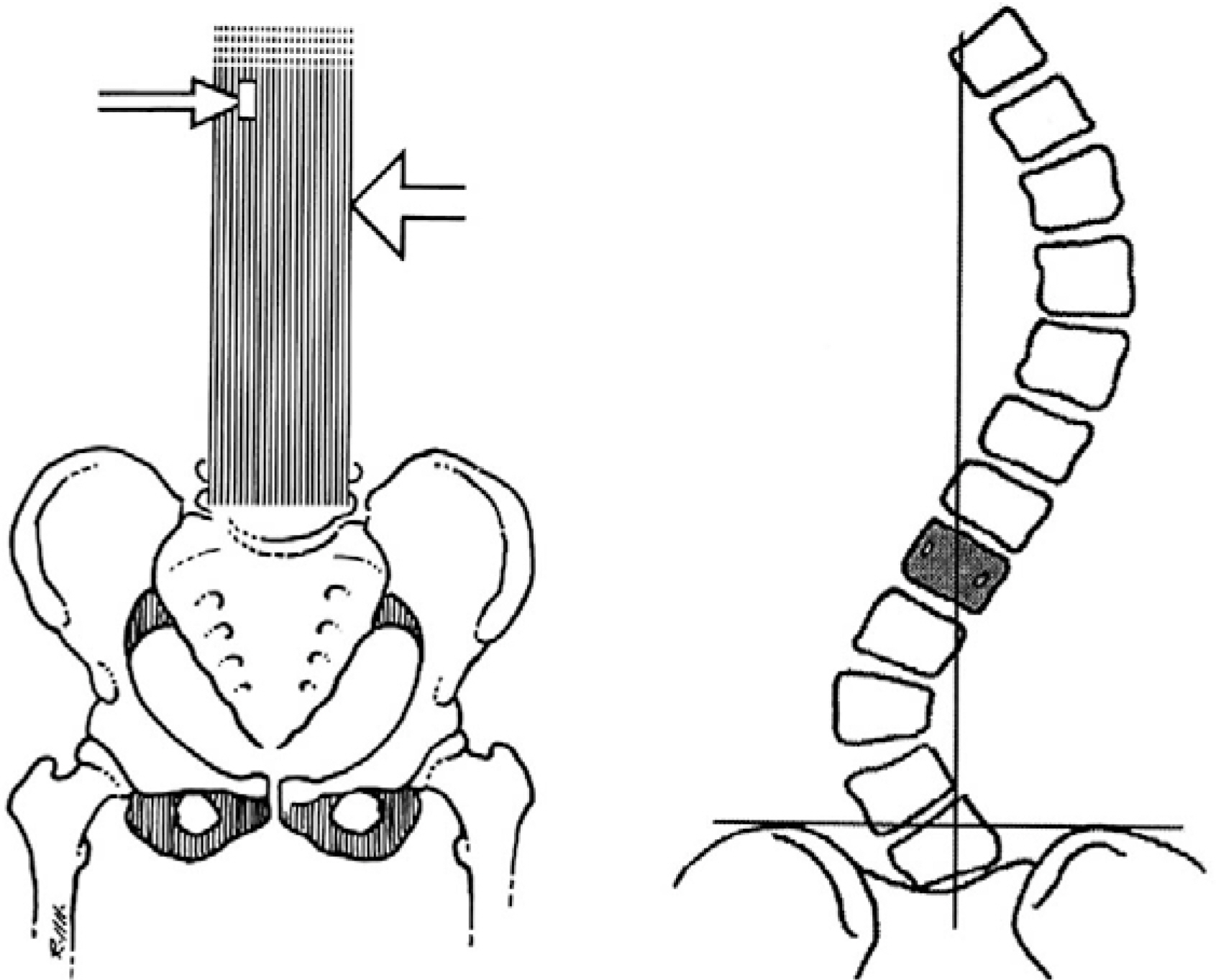
Fig. 1. (A) The stable zone of Harrington, defined by parallel lines drawn through the lumbosacral facets. the vertebral bodies within the lines are in the stable zone. (B) stable vertebra
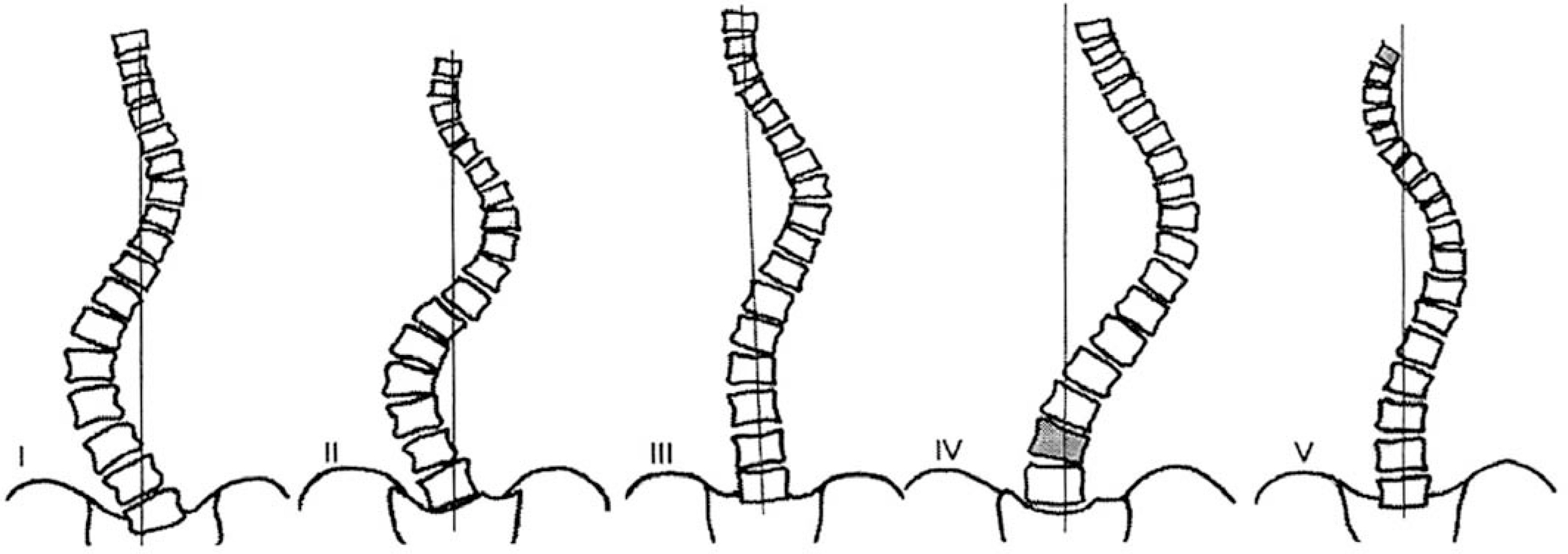
Fig. 2. King and Moe Classsification : Curve patterns

Fig. 3. King type 1: Lumbar curve is larger than thoracic curve on standing radiography and more rigid than thoracic curve. Fusion of both curves was done.

Fig. 4. King type 2: The rigid thoracic curve, from T5 to T10, is more rigid and larger than lumbar curve. Selective thoracic fusion was done from T4 to T11.
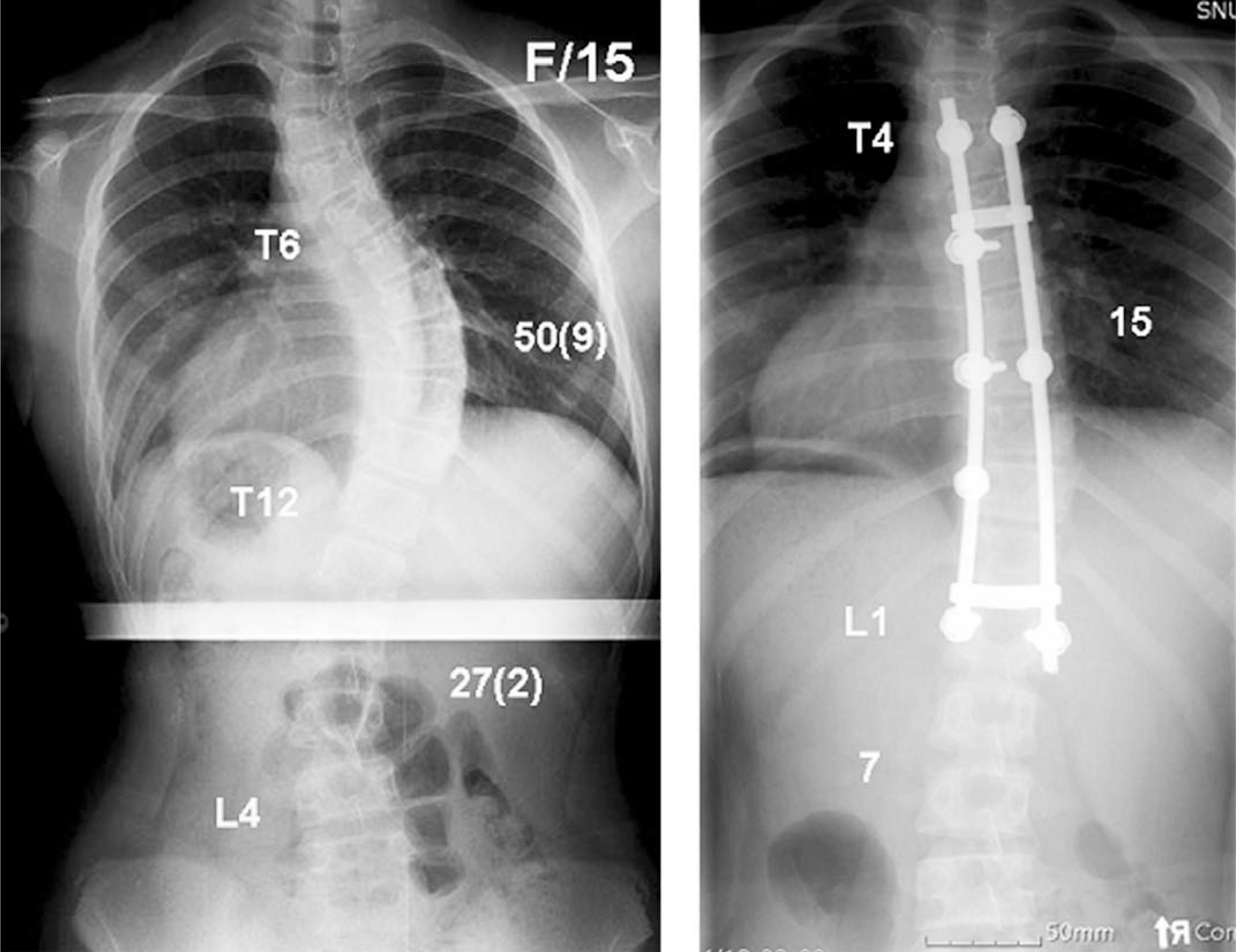
Fig. 5. King type 3: The right thoracic curve, from T6 to T12, measures 50 degrees. the lumbar curve is compensatory curve and doesn’ t cross the midline. Selective thoracic fusion was done to the neutral vertebra(L1).
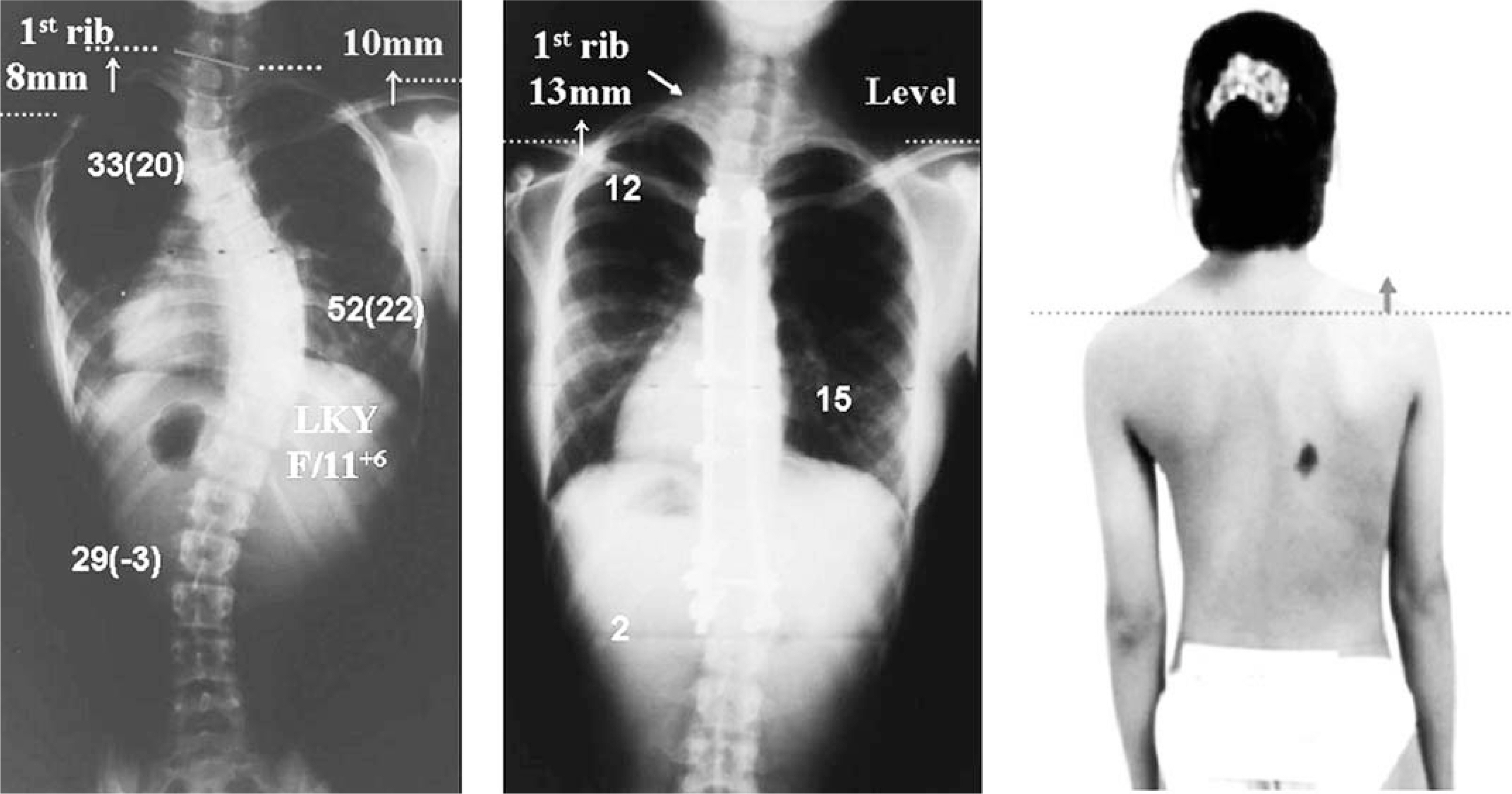
Fig. 6. King type 5: The first thoracic vertebra is tilted into the upper thoracic curve(called a positive T1 tilt) and the first rib is ele-vated on the convexity of the thoracic curve. Only lower thoracic curve was fused

Fig. 7. Double thoracic curves: The proximal thoracic curve is larger and more rigid than the lower thoracic curve, but in Lenke classification, the proximal thoracic curve cannot be the main curve.

Fig. 8. T1 tilt does not correlate well with left shoulder elevation, but correlates with left first rib elevation and trapezius prominence. T1 tilt and left first rib elevation should be considered as the indication of the extension of fusion to upper curve.
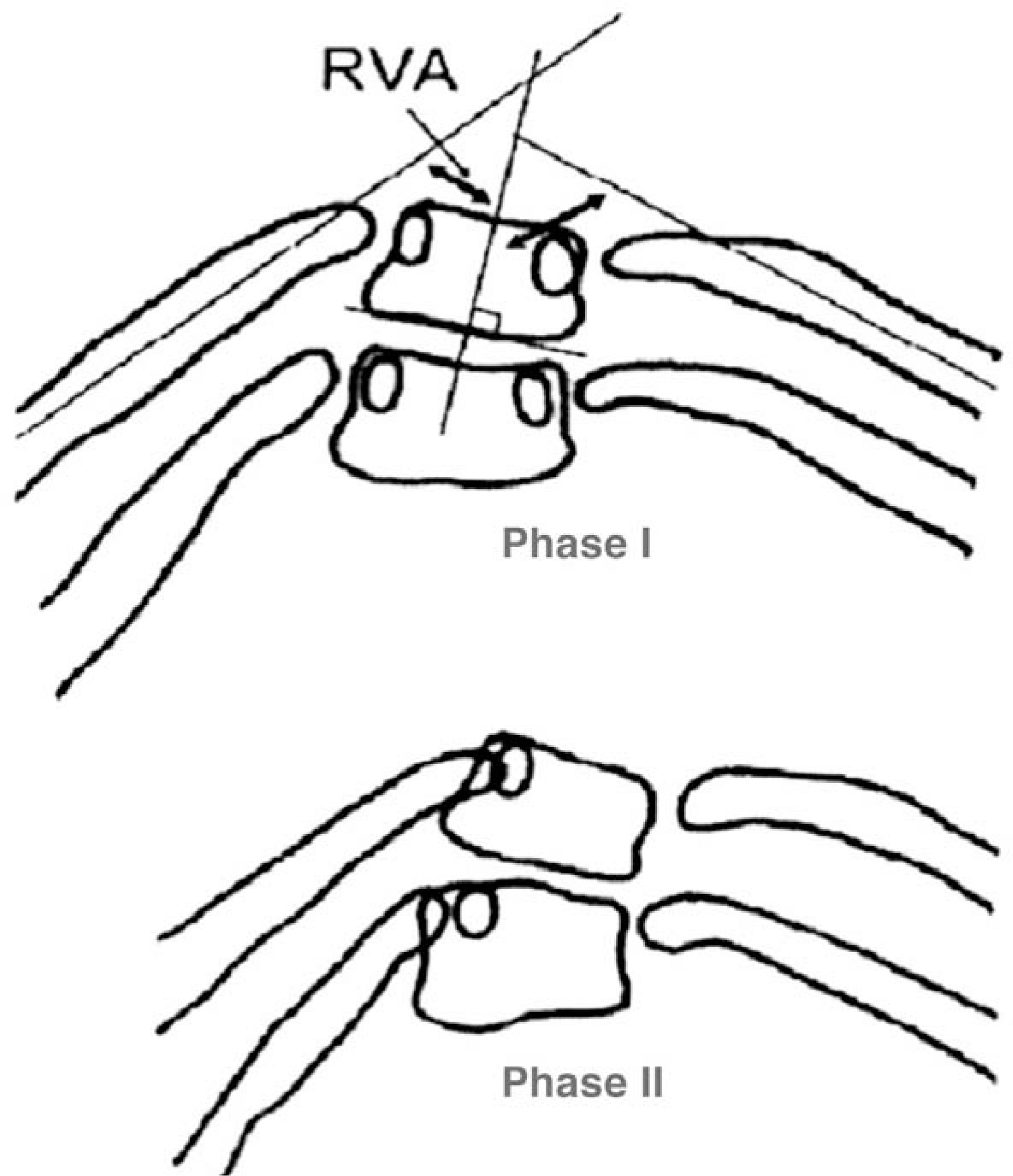
Fig. 9. Rib-vertebral angle difference
Cited by 1 articles
-
The relation between idiopathic scoliosis and the frontal and lateral facial form
Tae-Hwan Kim, Joo-Hwan Kim, Yae-Jin Kim, Il-Sik Cho, Yong-Kyu Lim, Dong-Yul Lee
Korean J Orthod. 2014;44(5):254-262. doi: 10.4041/kjod.2014.44.5.254.
Reference
-
1). Figueriedo UM, James AIP. Juvenile idiopathic scoliosis. J Bone Joint Surg. 1981; 63-B:61–66.2). King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg. 1983; 65-A:1302–1313.
Article3). Lee CK, Denis F, Winter RB, Lonstein JE. Analysis of the upper thoracic curve in surgically treated idiopathic scoliosis. Spine. 1993; 18:1599–1608.
Article4). Lee DH, Lee JC, Kim SH, Lim ST, Chang BS, Lee CK. Tactics for surgical treatment of the double thoracic scoliosis: Significance of T1 tilt, first rib elevation and correction ratio. J Korean Spine Surg. 2002; 9(2):106–114.5). Lenke LG, Betz RR, Clement D, Merola A, Haher TR, Lowe T, et al. Curve prevalence of a new classification of operative adolescent idiopathic scoliosis. Spine. 2002; 27:604–611.
Article6). Lenke LG, Betz RR, Haher TR, Lapp MA, Merola AA, Harms J, et al. Multisurgeon assesment of surgical decision-making in Adolescent idiopathic scoliosis. Curve classification, operative approach, and fusion levels. Spine. 2001; 26:2347–2353.7). Lenke LG, Betz RR, Harms J, Bridwell KH, Clement D, Lowe T, et al. Adolescent idiopathic scoliosis. A new classification to determine extent of spinal arthrodesis. J Bone Joint Surg. 2001; 83-A:1169–1181.8). Mehta MH. The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg. 1973; 55-B:513–520.
Article9). Puno RM, An KC, Puno RL, Jacob A, Chung SS. Treatment recommendation for idiopathic scoliosis. An assessment of the Lenke classification. Spine. 2003; 28:2102–2115.10). Richard BS, Sucato DJ, Konigsberg DE, Ouellet JA. Comparision of reliabilty between the Lenke and King Classification systems for adolescent idiopathic scoliosis using radiographs that were not premeasured. Spine. 2003; 28:1148–1157.11). Sanders AE, Baumann R, Brown H, Johnston CE, Lenke LG, Sink E. Selective anterior fusion of thoracolumbar/lumbar curves in adolescent. Spine. 2003; 28:484–491.12). Suk SI. Introduction of spinal deformity and idiopathic scoliosis. Spinal surgery. 2nd ed, Seoul, Newest Medical Publishing. 2004; Co:311–361.13). Suk SI, Chung ER, Lee JH, Kim JH, Lee SM, Lee JH, et al. Segmental pedicle screw fixation in thoracolumbar or lumbar idiopathic scoliosis. J Korean Orthop Assoc. 2003; 38:665–671.
Article14). Suk SI, Kim WJ, Lee CS, Lee SM, Kim JH, Chung ER, et al. Indication of proximal thoracic curve fusion in thoracic adolescent idiopathic scoliosis. Spine. 2000; 25:2342–2349.15). Suk SI, Lee SM, Chung ER, Kim JH, Kim WJ, Sohn HM. Determination of distal fusion level with segmental pedicle screw fixation in single thoracic idiopathic scoliosis. Spine. 2003; 28:484–491.
Article16). Suk SI, Lee SM, Kim JH, Kim WJ, Chung ER, Nah KH, et al. Decompensation in selective thoracic fusion by segmental pedicle screw fixation in King type II adolescent idiopathic scoliosis: Causative factors and its prevention. J Korean Spine Surg. 2000; 7(4):571–578.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An analysis of adolescent idiopathic scoliosis according to Coonrad classification
- The relation between idiopathic scoliosis and the frontal and lateral facial form
- A Clinical Study of Scoliosis
- Medical genomic approach to early-onset scoliosis
- Spontaneous Rib Fracture during Boston Brace Treatment for Adolescent Idiopathic Scoliosis
