Sentinel Lymph Node Biopsy in the Oral Cavity Cancer
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. chbaek@skku.edu
- KMID: 1505102
- DOI: http://doi.org/10.7599/hmr.2009.29.3.255
Abstract
- Elective neck dissection for the clinically node-negative neck is targeted to diagnose and eradicate the occult lymph node metastasis. However, this elective neck dissection gives unnecessary risk of complication and morbidity. Therefore, the extent of the elective neck dissection tends to be reduced to minimize the postoperative morbidity. The sentinel lymph node biopsy has been developed for this purpose. Sentinel lymph node is the first lymph node that gets lymphatic drainage from the tumor. Evaluation of this sentinel lymph node enables the prediction of the presence of occult lymph node metastasis. If the biopsy of the sentinel lymph node shows no metastasis, additional neck dissection can be avoided, which reduces the postoperative morbidity. There have been clinical studies on the sentinel lymph node biopsy for the head and neck squamous cell carcinoma, in which the diagnostic accuracy has been reported to be 95-100%. We started sentinel lymph node biopsy for the clinically node-negative, early-staged oral cavity cancer in December 2002. From 2002 to 2004, we evaluated its diagnostic accuracy. The positive predictive value and the negative predictive value were 100% and 98.5%, respectively. We currently determine the elective neck dissection according to the result of the sentinel lymph node biopsy.
MeSH Terms
Figure
-
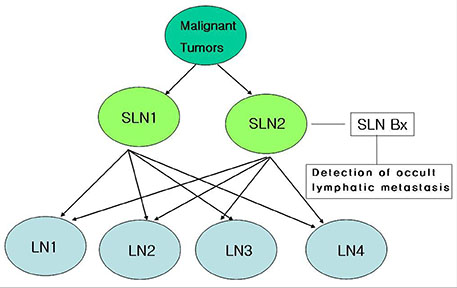
Fig. 1 Diagram presenting the concept of sentinel lymph node. Sentinel lymph node biopsy lead us to know whether metastases are present in the first echelon of draining lymph nodes.
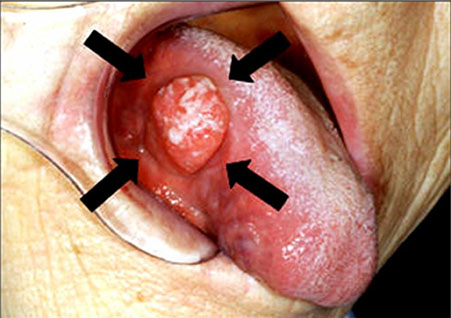
Fig. 2 The peritumoral injection of the radioacitive tracer.
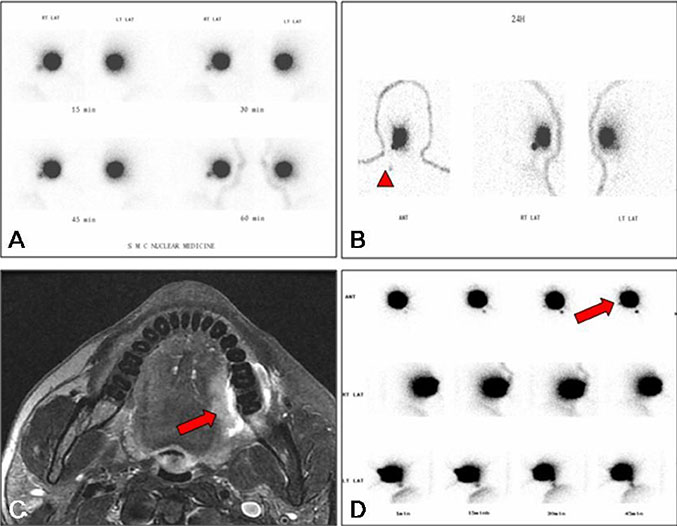
Fig. 3 Lymphoscintigraphy of a 56 year-old male patient with tongue cancer (pT1N1M0). (A) Early dynamic imaging presented sentinel lymph node at right level II immediately after the injection of radioactive tracer. Sentinel lymph node was visualized as late as 4 hours after the injection (arrowhead. C-D. A 72 year-old male patient with tongue cancer (pT2N0M0). (C) Preoperative MRI showed well-enhancing lesion at the left tongue. (D) At early dynamic lymphoscintigraphy revealed sentinel lymph nodes at right level II as well as left level II and III.
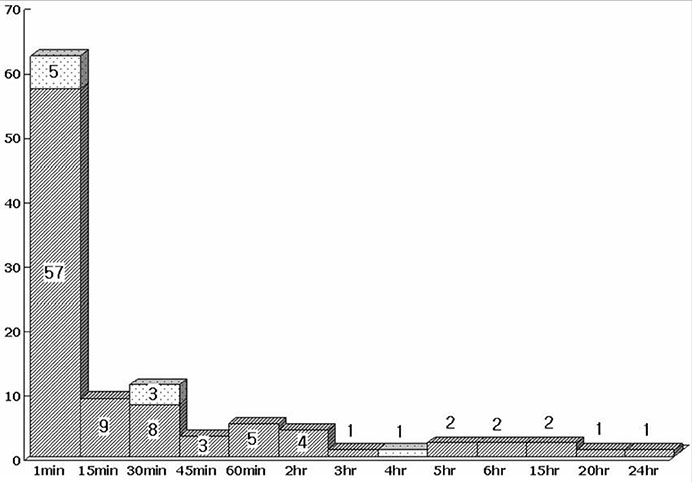
Fig. 4 Distribution of sentinel lymph nodes according to the time in lymphoscintigraphy.

Fig. 5 The handheld gamma probe (Navigator GPS, Tyco Health Care, USA).
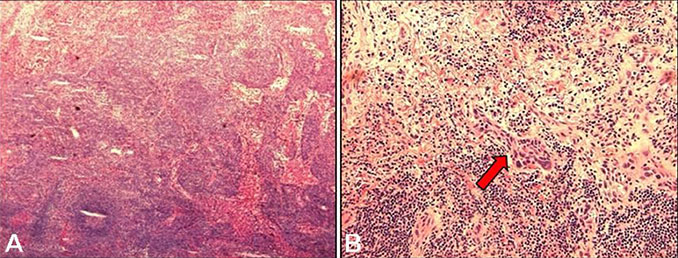
Fig. 6 Pathology of a sentinel lymph node. (A) In frozen biopsy, no tumor cell was found. Magnification ×40. (B) But, in permanent biopsy, small tumor cell nest was detected (arrow). Magnification ×400.
Reference
-
1. Hart RD, Nasser JG, Trites JR, Taylor SM, Bullock M, Barnes D. Sentinel lymph node biopsy in N0 squamous cell carcinoma of the oral cavity and oropharynx. Arch Otolaryngol Head Neck Surg. 2005; 131:34–38.
Article2. Jalisi S. Management of the clinically negative neck in early squamous cell carcinoma of the oral cavity. Otolaryngol Clin North Am. 2005; 38:37–46. viii
Article3. Hyde NC, Prvulovich E, Newman L, Waddington WA, Visvikis D, Ell P. A new approach to pre-treatment assessment of the N0 neck in oral squamous cell carcinoma: the role of sentinel node biopsy and positron emission tomography. Oral Oncol. 2003; 39:350–360.
Article4. Werner JA, Dunne AA, Ramaswamy A, Dalchow C, Behr T, Moll R, et al. The sentinel node concept in head and neck cancer: solution for the controversies in the N0 neck? Head Neck. 2004; 26:603–611.
Article5. Mendenhall WM, Million RR, Cassisi NJ. Elective neck irradiation in squamous-cell carcinoma of the head and neck. Head Neck Surg. 1980; 3:15–20.
Article6. Buckley JG, Feber T. Surgical treatment of cervical node metastases from squamous carcinoma of the upper aerodigestive tract: evaluation of the evidence for modifications of neck dissection. Head Neck. 2001; 23:907–915.
Article7. Pitman KT, Johnson JT, Myers EN. Effectiveness of selective neck dissection for management of the clinically negative neck. Arch Otolaryngol Head Neck Surg. 1997; 123:917–922.
Article8. Hosal AS, Carrau RL, Johnson JT, Myers EN. Selective neck dissection in the management of the clinically node-negative neck. Laryngoscope. 2000; 110:2037–2040.
Article9. Byers RM, Weber RS, Andrews T, McGill D, Kare R, Wolf P. Frequency and therapeutic implications of "skip metastases" in the neck from squamous carcinoma of the oral tongue. Head Neck. 1997; 19:14–19.
Article10. Ferlito A, Mannara GM, Rinaldo A, Politi M, Robiony M, Costa F. Is extended selective supraomohyoid neck dissection indicated for treatment of oral cancer with clinically negative neck? Acta Otolaryngol. 2000; 120:792–795.
Article11. Goyal A, Mansel RE. Current status of sentinel lymph node biopsy in solid malignancies. World J Surg Oncol. 2004; 2:9.12. Mamelle G. Selective neck dissection and sentinel node biopsy in head and neck squamous cell carcinomas. Recent Results Cancer Res. 2000; 157:193–200.
Article13. Alex JC, Sasaki CT, Krag DN, Wenig B, Pyle PB. Sentinel lymph node radiolocalization in head and neck squamous cell carcinoma. Laryngoscope. 2000; 110:198–203.
Article14. Alex JC. The application of sentinel node radiolocalization to solid tumors of the head and neck: a 10-year experience. Laryngoscope. 2004; 114:2–19.
Article15. Minamikawa T, Umeda M, Komori T. Reliability of sentinel lymph node biopsy with squamous cell carcinoma of the oral cavity. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 99:532–538. discussion 9-41.
Article16. Tschopp L, Nuyens M, Stauffer E, Krause T, Zbaren P. The value of frozen section analysis of the sentinel lymph node in clinically N0 squamous cell carcinoma of the oral cavity and oropharynx. Otolaryngol Head Neck Surg. 2005; 132:99–102.
Article17. Koch WM, Choti MA, Civelek AC, Eisele DW, Saunders JR. Gamma probe-directed biopsy of the sentinel node in oral squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 1998; 124:455–459.
Article18. Stoeckli SJ, Pfaltz M, Ross GL, Steinert HC, MacDonald DG, Wittekind C, Soutar DS. The second international conference on sentinel node biopsy in mucosal head and neck cancer. Ann Surg Oncol. 2005; 12:919–924.
Article19. Jeong HS, Baek CH, Son YI, Cho DY, Chung MK, Min JY, Ko YH, Kim BT. Sentinel lymph node radiolocalization with 99mTc filtered tin colloid in clinically node-negative squamous cell carcinomas of the oral cavity. J Korean Med Sci. 2006; 21:865–870.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Number of Removed Lymph Nodes for an Acceptable False Negative Rate in Sentinel Lymph Node Biopsy for Breast Cancer
- Validation and Controversy of Sentinel Node Biopsy for Breast Cancer
- Sentinel Lymph Node Biopsy in Breast Cancer: A Clinical Review and Update
- Minimally Invasive Surgery Based on Sentinel Node Biopsy for Gastrointestinal Cancer
- Clinical relevance of sentinel lymph node biopsy in early ovarian cancer
