Yonsei Med J.
2013 Mar;54(2):464-468. 10.3349/ymj.2013.54.2.464.
Easily Removable Ureteral Catheters for Internal Drainage in Children: A Preliminary Report
- Affiliations
-
- 1Department of Urology, Jeju National University College of Medicine, Jeju, Korea.
- 2Department of Urology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. chhong52@yuhs.ac
- 3Department of Urology, Uijeongbu St. Mary's Hospital, The Catholic University of Korea College of Medicine, Uijeongbu, Korea.
- KMID: 1503911
- DOI: http://doi.org/10.3349/ymj.2013.54.2.464
Abstract
- PURPOSE
We review our experience using a new and easily removable ureteral catheter in patients who underwent complicated ureteral reimplantation. Our goal was to shorten hospital stay and lower anxiety during catheter removal without fear of postoperative ureteral obstruction.
MATERIALS AND METHODS
Between April 2009 and September 2010, nine patients who underwent our new method of catheter removal after ureteral reimplantation were enrolled. Patients who underwent simple ureteral reimplantation were excluded from the study. Following ureteral reimplantation, a combined drainage system consisting of a suprapubic cystostomy catheter and a ureteral catheter was installed. Proximal external tubing was clamped with a Hem-o-lok clamp and the rest of the external tubing was eliminated. Data concerning the age and sex of each patient, reason for operation, method of ureteral reimplantation, and postoperative parameters such as length of hospital stay and complications were recorded.
RESULTS
Of the nine patients, four had refluxing megaureter, four had a solitary or non-functional contralateral kidney and one had ureteral stricture due to a previous anti-reflux operation. The catheter was removed at postoperative week one. The mean postoperative hospital stay was 2.4 days (range 1-4 days), and the mean follow-up was 9.8 months. None of the patients had postoperative ureteral obstructions, and there were no cases of migration or dislodgement of the catheter.
CONCLUSION
Our new method for removing the ureteral catheter would shorten hospital stays and lower levels of anxiety when removing ureteral catheters in patients with a high risk of postoperative ureteral obstruction.
MeSH Terms
Figure
-
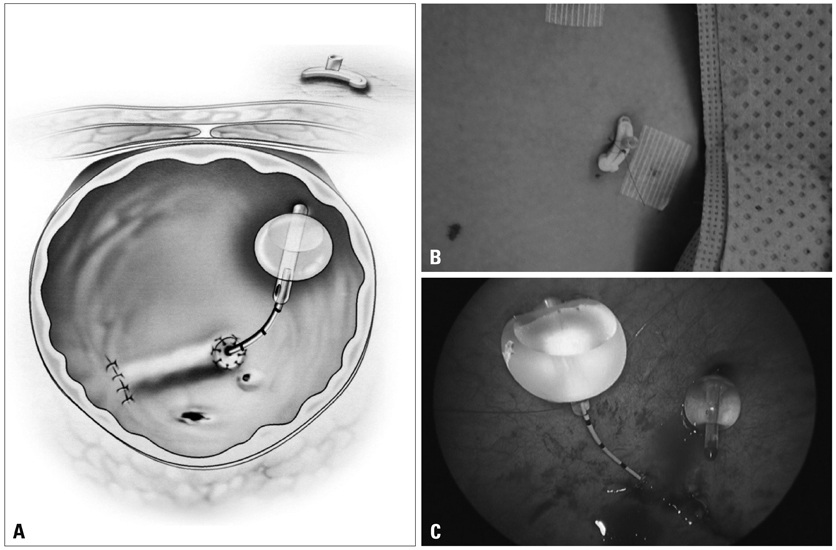
Fig. 1 (A) Schematic illustration of our new internal drainage system. (B) Hem-o-lok clamp holding the suprapubic catheter without an external drainage system. (C) The ureteral catheter and suprapubic cystostomy catheter are positioned, and the ureteral catheter is fixed to the drainage hole at the distal end of the cystostomy catheter using a nylon 4-0 suture.
Reference
-
1. Brandell RA, Brock JW 3rd. Ureteral reimplantation: postoperative management without catheters. Urology. 1993. 42:705–707.
Article2. Miller OF, Bloom TL, Smith LJ, McAleer IM, Kaplan GW, Kolon TF. Early hospital discharge for intravesical ureteroneocystostomy. J Urol. 2002. 167:2556–2559.
Article3. Hong CH, Kim JH, Jung HJ, Im YJ, Han SW. Single-surgeon experience with transvesicoscopic ureteral reimplantation in children with vesicoureteral reflux. Urology. 2011. 77:1465–1469.
Article4. Bregg K, Riehle RA Jr. Morbidity associated with indwelling internal ureteral stents after shock wave lithotripsy. J Urol. 1989. 141:510–512.
Article5. Barbour KW, Arunachalam P, King PA, McAndrew HF. The use of ureteral stents and suprapubic catheter in vesicoureteric reflux surgery. Pediatr Surg Int. 2004. 20:387–388.
Article6. Taveres A, Manaboriboon N, Lorenzo AJ, Farhat WA. Insertion of an internal-external nephroureteral stent during pediatric laparoscopic pyeloplasty: description of the technique. Urology. 2008. 71:1199–1202.
Article7. Kennelly MJ, Bloom DA, Ritchey ML, Panzl AC. Outcome analysis of bilateral Cohen cross-trigonal ureteroneocystostomy. Urology. 1995. 46:393–395.
Article8. Flickinger JE, Trusler L, Brock JW 3rd. Clinical care pathway for the management of ureteroneocystostomy in the pediatric urology population. J Urol. 1997. 158(3 Pt 2):1221–1225.
Article9. Jarvis WR. Controlling healthcare-associated infections: the role of infection control and antimicrobial use practices. Semin Pediatr Infect Dis. 2004. 15:30–40.
Article10. Festini F, Cocchi P, Mambretti D, Tagliabue B, Carotti M, Ciofi D, et al. Nosocomial Rotavirus Gastroenteritis in pediatric patients: a multi-center prospective cohort study. BMC Infect Dis. 2010. 10:235.
Article11. Zhang Q, Xu X, Langley JM, Zhu B, Zhang N, Tang Y. Health-associated infections in a pediatric nephrology unit in China. Am J Infect Control. 2010. 38:473–475.
Article12. Spencer JD, Schwaderer A, McHugh K, Hains DS. Pediatric urinary tract infections: an analysis of hospitalizations, charges, and costs in the USA. Pediatr Nephrol. 2010. 25:2469–2475.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Experience with preliminary percutaneous nephrostomy in pediatric hydronephrosis
- Management of Iatrogenic Ureteral Injury
- Clinical Observation on Surgical Ureteral Injuries
- Extravesical Repair of Primary Vesicoureteral Reflux with Detrusorr- haphy
- Can Endoscopic Nasobiliary Drainage Involving Two Catheters Be Used to Treat Various Conditions?
