Blepharoptosis Repair through the Small Orbital Septum Incision and Minimal Dissection Technique in Patients with Coexisting Dermatochalasis
- Affiliations
-
- 1Department of Ophthalmology, St. Vincent's Hospital, The Catholic University of Korea College of Medicine, Suwon, Korea. laty@catholic.ac.kr
- KMID: 1501788
- DOI: http://doi.org/10.3341/kjo.2013.27.1.1
Abstract
- PURPOSE
To describe a modified surgical technique for blepharoptosis repair through a small orbital septum incision and minimal dissection, along with the results obtained in patients with coexisting dermatochalasis.
METHODS
A retrospective chart review included 33 patients (52 eyelids) with blepharoptosis coexisting with dermatochalasis, surgically corrected through a small orbital septum incision and minimal dissection after redundant upper lid skin excision, by placing a single fixation suture between the levator aponeurosis and the tarsal plate. Outcome measures included the pre- and postoperative marginal reflex distances (MRD1), eyelid contour, post-operative complications, and need for reoperation.
RESULTS
The pre- and postoperative MRD1 averaged 1.1 +/- 0.8 mm and 2.8 +/- 1.1 mm, respectively. Of the 33 patients, 9 patients (9 eyelids) underwent surgery on one eyelid for unilateral blepharoptosis and dermatochalasis (Group I), 5 patients (5 eyelids) underwent a simple skin excision blepharoplasty of the contralateral eyelid (Group II), and 19 patients (38 eyelids) underwent bilateral blepharoptosis and dermatochalasis repair (Group III). Of the 14 eyelids that underwent unilateral ptosis repair (Groups I and II), 12 eyelids (85.7%) showed less than a 1-mm difference from the contralateral eyelid. Of the 38 eyelids that underwent bilateral ptosis repair (Group III), 27 eyelids (71.1%), 5 eyelids (13.1%), and 6 eyelids (15.8%) had excellent, good, and poor outcomes, respectively. Overall, 44 eyelids (84.6%) out of a total of 52 eyelids had successful outcomes; the remaining 8 eyelids demonstrated unsatisfactory eyelid contour was corrected by an additional surgery.
CONCLUSIONS
Blepharoptosis repair through a small orbital septum incision and minimal dissection can be considered an efficient technique in patients with ptosis and dermatochalasis.
MeSH Terms
Figure
-
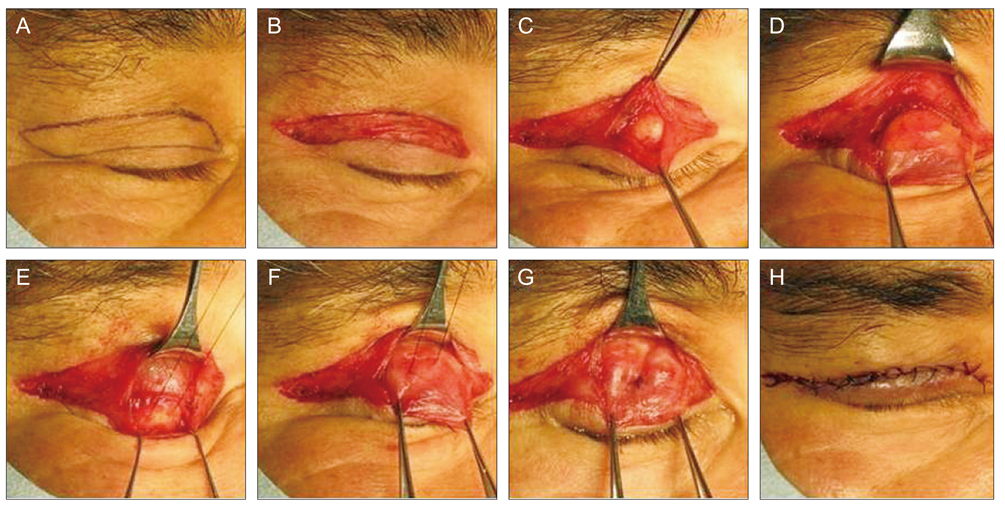
Fig. 1 Procedure for blepharoptosis correction and redundant skin excision through the small orbital septum incision and minimal dissection technique. (A) A skin marking was made along the natural lid crease line and the redundant skin to be excised was designed. (B) The redundant skin and the underlying orbicularis muscle were excised. (C) After incising the orbital septum for about a length of 10 mm just above the tarsal plate, the pretarsal orbicularis muscle was dissected until the tarsal plate was exposed across the same width. (D) By dissecting in an upward direction from the tarsal plate, the preaponeurotic fat pad was identified and the levator aponeurosis was exposed till the level of musculo-aponeurotic junction. (E) A partial thickness suture of more than 5 mm in width was placed through the tarsal plate in a horizontal fashion. (F) A double-armed, non-absorbable suture was passed through the levator aponeurosis at a predetermined position. (G) The permanent fixation suture was tied down after inspecting the eyelid height and contour. (H) Finally, the skin was closed with interrupted sutures of 6-0 black silk.
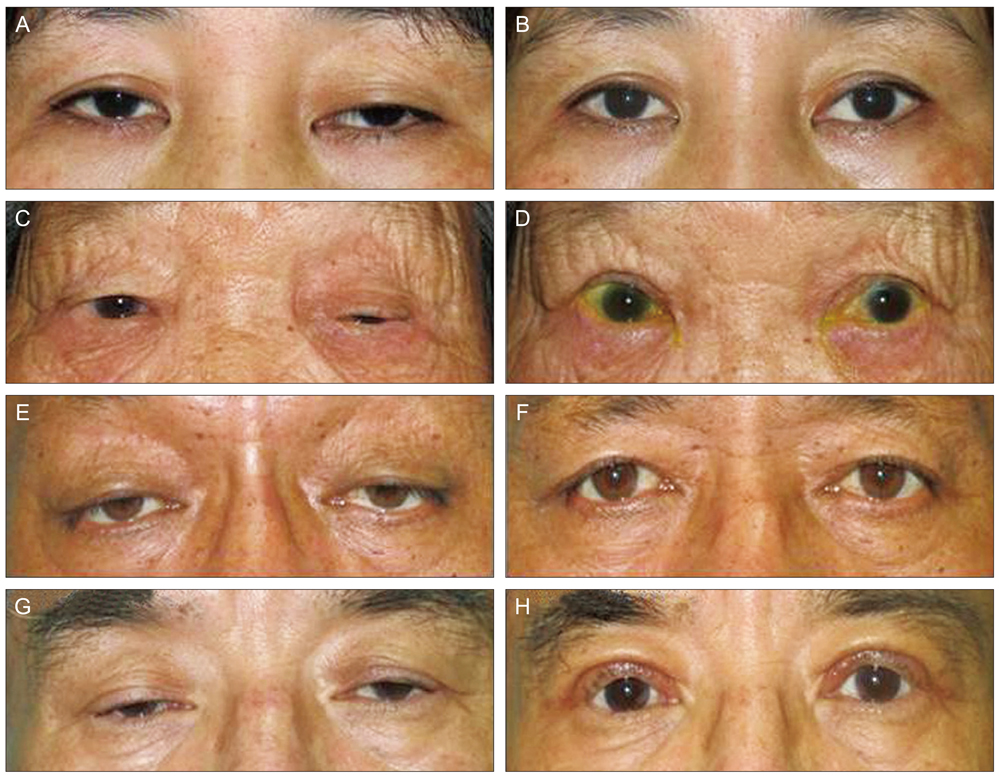
Fig. 2 Preoperative and postoperative photographs of patient (at 2 months). Preoperative (A) and postoperative (B) pictures of a patient from Group I (left eye). Preoperative (C) and postoperative (D) pictures of a patient from Group II (left eye). Preoperative (E,G) and postoperative (F,H) pictures of patients from Group III, respectively. Group I: operation for unilateral ptosis and dermatochalasis. Group II: operation for unilateral ptosis and dermatochalasis + redundant skin excision only of contralateral eyelid. Group III: operation for bilateral ptosis and dermatochalasis.
Reference
-
1. Waqar S, McMurray C, Madge SN. Transcutaneous blepharoptosis surgery-advancement of levator aponeurosis. Open Ophthalmol J. 2010. 4:76–80.2. Lucarelli MJ, Lemke BN. Small incision external levator repair: technique and early results. Am J Ophthalmol. 1999. 127:637–644.3. Baroody M, Holds JB, Sakamoto DK, et al. Small incision transcutaneous levator aponeurotic repair for blepharoptosis. Ann Plast Surg. 2004. 52:558–561.4. Bernardini FP, de Conciliis C, Devoto MH. Mini-invasive ptosis surgery. Orbit. 2006. 25:111–115.5. Frueh BR, Musch DC, McDonald H. Efficacy and efficiency of a new involutional ptosis correction procedure compared to a traditional aponeurotic approach. Trans Am Ophthalmol Soc. 2004. 102:199–206.6. Frueh BR, Musch DC, McDonald HM. Efficacy and efficiency of a small-incision, minimal dissection procedure versus a traditional approach for correcting aponeurotic ptosis. Ophthalmology. 2004. 111:2158–2163.7. Dresner S. Chen WP, editor. Ptosis management: a practical approach. Oculoplastic surgery: the essentials. 2001. New York: Thieme;75–88.8. Liu D. Ptosis repair by single suture aponeurotic tuck: surgical technique and long-term results. Ophthalmology. 1993. 100:251–259.9. Baek SH, Park MS, Park HJ. The effect of simplified single suture aponeurotic tuck in ptosis patients. J Korean Ophthalmol Soc. 2003. 44:1011–1016.10. Meltzer MA, Elahi E, Taupeka P, Flores E. A simplified technique of ptosis repair using a single adjustable suture. Ophthalmology. 2001. 108:1889–1892.11. Lee TS, Nam DH. Surgical results of modified Fasanella-Servat operation. J Korean Ophthalmol Soc. 1999. 40:248–252.12. Moon HS, Lee JH, Baek SH. The frontalis sling operation using preserved fascia lata: modified Crawford technique. J Korean Ophthalmol Soc. 2005. 46:10–15.13. Carter SR, Meecham WJ, Seiff SR. Silicone frontalis slings for the correction of blepharoptosis: indications and efficacy. Ophthalmology. 1996. 103:623–630.14. Jeong S. Clinical study of simple levator resection in ptosis patients. J Korean Ophthalmol Soc. 2002. 43:551–555.15. Chang DJ, La TY. Blepharoptosis repair by small cutaneous incision and minimal dissection technique. J Korean Ophthalmol Soc. 2009. 50:1146–1151.16. McCulley TJ, Kersten RC, Kulwin DR, Feuer WJ. Outcome and influencing factors of external levator palpebrae superioris aponeurosis advancement for blepharoptosis. Ophthal Plast Reconstr Surg. 2003. 19:388–393.17. Bartley GB, Lowry JC, Hodge DO. Results of levator-advancement blepharoptosis repair using a standard protocol: effect of epinephrine-induced eyelid position change. Trans Am Ophthalmol Soc. 1996. 94:165–173.18. Li J, Lin M, Zhou H, et al. Double-eyelid blepharoplasty incorporating blepharoptosis surgery for 'latent' aponeurotic ptosis. J Plast Reconstr Aesthet Surg. 2011. 64:993–999.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Blepharoptosis Repair by Small Cutaneous Incision and Minimal Dissection Technique
- Correction of the Sunken Upper Eyelid Depending on the Dermatochalasis or Blepharoptosis Using the Autologous Fat Grafting
- Infrabrow excision with septo-myocutaneous flap repositioning in aged eyelids in Asians
- Correction of Blepharoptosis using Posterior Check Ligament Sling
- Correction of blepharoptosis by a composite flap procedure utilizing the orbicularis oculi muscle and orbital septum
