Repeatedly Recurrent Colon Cancer Involving the Appendiceal Orifice after Endoscopic Piecemeal Mucosal Resection: A Case Report
- Affiliations
-
- 1Endoscopy Division, National Cancer Center Hospital, Tokyo, Japan. tamatsud@ncc.go.jp
- 2Molecular Pathology Division, National Cancer Center Research Institute, Tokyo, Japan.
- 3Pathology Division, National Cancer Center Hospital, Tokyo, Japan.
- 4Colorectal Surgical Division, National Cancer Center Hospital, Tokyo, Japan.
- KMID: 1501652
- DOI: http://doi.org/10.4166/kjg.2013.61.5.286
Abstract
- Local recurrence after endoscopic piecemeal mucosal resection (EPMR) for colorectal tumors is a crucial issue. However, such recurrence is usually detected within one year and cured with additional endoscopic treatment, which makes EPMR acceptable. Herein, we report a rare case of repeatedly recurrent colon cancer involving the appendiceal orifice after EPMR, which was not cured with additional endoscopic treatments. A 67-year-old man was referred to us for endoscopic treatment of a 25 mm cecal tumor spreading to the appendiceal orifice in May 2002. The tumor was resected with EPMR, showing well differentiated intramucosal adenocarcinoma with a positive lateral cut margin of tubular adenoma. Endoscopic surveillance was conducted and the first local recurrence was detected in August 2006. Although we resected it endoscopically, the second local recurrence was found in September 2007 and we removed it with endoscopic resection again. However, the third local recurrence was detected in March 2008. Although endoscopic resection was performed also for the third recurrence, curative resection was not achieved. In February 2009, laparoscopic assisted colectomy was performed and histopathological examination showed well differentiated adenocarcinoma with deep submucosal invasion. This case is important in considering indication for endoscopic resection in colorectal tumors involving the appendiceal orifice.
Keyword
MeSH Terms
Figure
-
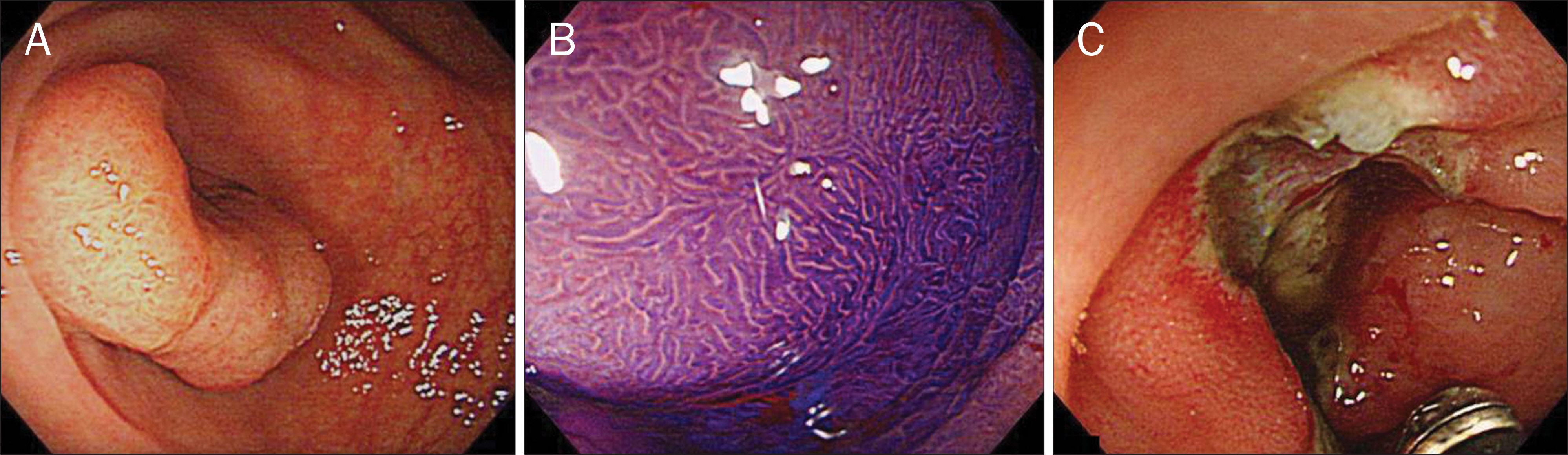
Fig. 1. (A) Conventional colonoscopy finding. A 25 mm cecal sessile tumor spreading to the appendiceal orifice was revealed. (B) Magnifying chromoendoscopy with crystal violet staining. A noninvasive pattern was disclosed. (C) Endoscopic finding after endoscopic piecemeal resection of the tumor showing macroscopically no residual tumor.

Fig. 2. (A) Follow-up colonoscopy finding. The third recurrent tumor, 10 mm in size, was detected at the site of the initial endoscopic piecemeal mucosal resection. (B) Magnifying chromoendoscopy with crystal violet staining. A noninvasive pattern was shown.

Fig. 3. (A) The surgically resected specimen. The recurrent tumor was seen in the appendiceal orifice (arrowheads). (B) Histopathological examination of surgically resected specimen. Well differentiated adenocarcinoma in the cecum and the appendix was revealed (H&E,×40). (C) The assessment of muscularis mucosae with desmin staining (arrowheads). The disruption of the muscularis mucosae and the submucosal invasion of the tumor were demonstrated (Desmin staining, ×40).
Reference
-
References
1. Tanaka S, Haruma K, Oka S, et al. Clinicopathologic features and endoscopic treatment of superficially spreading colorectal neoplasms larger than 20 mm. Gastrointest Endosc. 2001; 54:62–66.
Article2. Hurlstone DP, Sanders DS, Cross SS, et al. Colonoscopic resection of lateral spreading tumours: a prospective analysis of endoscopic mucosal resection. Gut. 2004; 53:1334–1339.
Article3. Hotta K, Fujii T, Saito Y, Matsuda T. Local recurrence after endoscopic resection of colorectal tumors. Int J Colorectal Dis. 2009; 24:225–230.
Article4. Saito Y, Fukuzawa M, Matsuda T, et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surg Endosc. 2010; 24:343–352.
Article5. Isomoto H, Nishiyama H, Yamaguchi N, et al. Clinicopathological factors associated with clinical outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms. Endoscopy. 2009; 41:679–683.
Article6. Fujishiro M, Yahagi N, Kakushima N, et al. Outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms in 200 consecutive cases. Clin Gastroenterol Hepatol. 2007; 5:678–683.
Article7. Tamegai Y, Saito Y, Masaki N, et al. Endoscopic submucosal dissection: a safe technique for colorectal tumors. Endoscopy. 2007; 39:418–422.
Article8. Saito Y, Uraoka T, Matsuda T, et al. Endoscopic treatment of large superficial colorectal tumors: a case series of 200 endoscopic submucosal dissections (with video). Gastrointest Endosc. 2007; 66:966–973.
Article9. Sakamoto T, Saito Y, Matsuda T, Fukunaga S, Nakajima T, Fujii T. Treatment strategy for recurrent or residual colorectal tumors after endoscopic resection. Surg Endosc. 2011; 25:255–260.
Article10. Matsuda T, Fujii T, Saito Y, et al. Efficacy of the invasive/noninvasive pattern by magnifying chromoendoscopy to estimate the depth of invasion of early colorectal neoplasms. Am J Gastroenterol. 2008; 103:2700–2706.
Article11. Khashab M, Eid E, Rusche M, Rex DK. Incidence and predictors of "late" recurrences after endoscopic piecemeal resection of large sessile adenomas. Gastrointest Endosc. 2009; 70:344–349.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Local recurrence and subsequent endoscopic treatment after endoscopic piecemeal mucosal resection with or without precutting in the colorectum
- Endoscopic Treatment for Superficial Nonampullary Duodenal Tumors
- Underwater Endoscopic Mucosal Resection without Submucosal Injection Facilitates En bloc Resection of Colon Adenomas Extending into a Diverticulum
- Re-Endoscopic Mucosal Resection for a Residual or Locally Recurrent Gastric Lesion after Endoscopic Mucosal Resection
- Natural Orifice Transluminal Endoscopic Surgery and Upper Gastrointestinal Tract
