A Case of Huge Thrombus in the Aortic Arch with Cerebrovascular Embolization
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, Yeungnam University, Daegu, Korea. grhong@med.yu.ac.kr
- KMID: 1473720
- DOI: http://doi.org/10.4250/jcu.2009.17.4.148
Abstract
- Pedunculated thrombus in the aortic arch that is associated with cerebral infarction is very rare requires prompt diagnosis and treatment to prevent occurrence of another devastating complication. Transesophageal echocardiography is useful for detecting source of embolism including aortic thrombi. The treatment options of aortic thrombi involves anticoagulation, thrombolysis, thromboaspiration, and thrombectomy. Here we report a case of huge thrombus in the aortic arch, resulting in acute multifocal cerebellar embolic infarct in patient without any risk factors for vascular thrombosis. Thrombi in the aortic arch were diagnosed by transesophageal echocardiography and treated with anticoagulants successfully.
Keyword
MeSH Terms
Figure
-

Fig. 1 Brain magnetic resonance imaging, acute infarct on right posterior internal communicating artery territory and multifocal cerebellum (arrow).
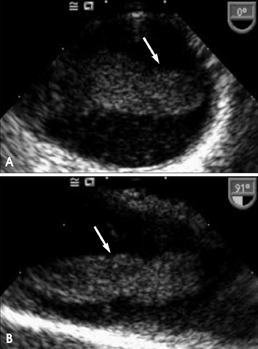
Fig. 2 Transesophageal echocardiogram demonstrates a large mobile protruding mass (arrow) in the aortic arch in transverse (A) and longitudinal (B) views.

Fig. 3 Multi-detector computed tomography scan demonstrate the mass in the aortic arch (arrow).
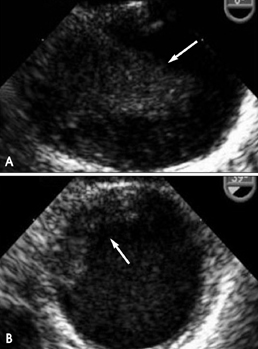
Fig. 4 Follow-up transesophageal echocardiogram shows small remnant thrombus in the base of atheromatous plaque (arrow)(B) compare with before anticoagulation therapy (arrow)(A).
Cited by 1 articles
-
Recurrent Cerebral Infarction Caused by Mobile Aortic Arch Thrombus Refractory to Warfarin Therapy
Soo-Kyung Bok, Young-Jin Lee, So-Young Ahn
Ann Rehabil Med. 2013;37(5):750-754. doi: 10.5535/arm.2013.37.5.750.
Reference
-
1. Panetta T, Thompson JE, Talkington CM, Garrett WV, Smith BL. Arterial embolectomy: a 34-year experience with 400 cases. Surg Clin North Am. 1986. 66:339–353.
Article2. Gagliardi JM, BattM , Khodja RH, Le bas P. Mural thrombus of the aorta. Ann Vasc Surg. 1988. 2:201–204.
Article3. Laperche T, Laurian C, Roudaut R, Steg PG. Mobile thromboses of the aortic arch without aortic debris. A transesophageal echocardiographic finding associated with unexplained arterial embolism. The Filiale Echocardiographie de la Société Française de Cardiologie. Circulation. 1997. 96:288–294.
Article4. Sadony V, Walz M, Löhr E, Rimpel J, Richter HJ. Unusual cause of recurrent arterial embolism: floating thrombus in the aortic arch surgically removed under hypothermic cardiocirculatory arrest. Eur J Car-diothorac Surg. 1988. 2:468–471.
Article5. Tunick PA, Kronzon I. Protruding atherosclerotic plaque in the aortic arch of patients with systemic embolization: a new finding seen by transesophageal echocardiography. Am Heart J. 1990. 120:658–660.
Article6. Rubin BG, Allen BT, Anderson CB, Barzilai B, Sicard GA. An embolizing lesion in a minimally diseased aorta. Surgery. 1992. 112:607–610.7. Machleder HI, Takiff H, Lois JF, Holburt E. Aortic mural thrombus: an occult source of arterial thromboembolism. J Vasc Surg. 1986. 4:473–478.
Article8. Lozano P, Gomez FT, Julia J, M-Rimbau E, Garcia F. Recurrent embolism caused by floating thrombus in the thoracic aorta. Ann Vasc Surg. 1998. 12:609–611.
Article9. Song Jin-Ho, Park Geung-Dong, Cho Gil-Hyun, Kim Doo-Il, Kim Dong-Soo. Cerebral infarction caused by floating thoracic aortic throm-bus in young male. J Cardiovascular Ultrasound. 2000. 8:236–240.
Article10. Blanchard DG, Kimura BJ, Dittrich HC, DeMaria AN. Transesophageal echocardiography of the aorta. JAMA. 1994. 272:546–551.
Article11. Wiet SP, Pearce WH, McCarthy WJ, Joob AW, Yao JS, McPherson DD. Utility of transesophageal echocardiography in the diagnosis of disease of the thoracic aorta. J Vasc Surg. 1994. 20:613–620.
Article12. Blackshear JL, Jahangir A, Oldenburg WA, Safford RE. Digital embolization from plaque-related thrombus in the thoracic aorta: identification with transesophageal echocardiography and resolution with warfarin therapy. Mayo Clin Proc. 1993. 68:268–272.
Article13. Culliford At, Tunick PA, Katz ES, Kronzon I, Galloway AC, Ribakove GH, Esposito RA, Spencer FC. Initial experience with removal of protruding atheroma from the aortic arch: diagnosis by transesophageal echo, operative technique, and follow-up [Abstract]. J Am Coll Cardiol. 1993. 21:342A.14. Lau LS, Blanchard DG, Hye RJ. Diagnosis and management of patients with peripheral macroemboli from thoracic aortic pathology. Ann Vasc Surg. 1997. 11:348–353.
Article15. Hahn TL, Dalsing MC, Sawchuk AP, Cikrit DF, Lalka SG. Primary aortic mural thrombus: presentation and treatment. Ann Vasc Surg. 1999. 13:52–59.
Article16. Reber PU, Patel AG, Stauffer E, Müller MF, Do DD, Kniemeyer HW. Mural aortic thrombi: An important cause of peripheral embolization. J Vasc Surg. 1999. 30:1084–1089.
Article17. Choukroun EM, Labrousse LM, Madonna FP, Deville C. Mobile thrombus of the thoracic aorta: diagnosis and treatment in 9 cases. Ann Vasc Surg. 2002. 16:714–722.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Floating Thrombus in Aortic Arch
- Successful Surgical Treatment of Trombus in the Aortic Arch
- Cerebral Embolic Infarction Caused by Aortic Arch Thrombus with Iron Deficiency Anemia
- A Case of Saccular Arteriosclerotic Aortic Aneurysm Associated with Thrombus in Aortic Arch
- Floating Thrombus in the Aortic Arch: A Case Report
