J Korean Endocr Soc.
2009 Jun;24(2):132-137. 10.3803/jkes.2009.24.2.132.
A Case of Pseudohypoparathyroidism without Albright's Hereditary Osteodystrophy in an Adult
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University of College of Medicine, Korea.
- KMID: 1468509
- DOI: http://doi.org/10.3803/jkes.2009.24.2.132
Abstract
- Pseudohypoparathyroidism is a rare disease caused by resistance to parathyroid hormone, and is associated with typical clinical typical symptoms such as tetany and seizures, hypocalcemia, hyperphosphatemia and increased parathyroid hormone levels. Pseudohypoparathyroidism is classified to Type Ia, Ib, Ic and II according to the clinical and biochemical manifestations. Type Ia and Ic have morphological characteristics called Albright's hereditary osteodystrophy. Type Ib differs from type II for the pathogenesis. Type Ib may~receptors and type II may~ pathway, but the pathophysiology of type II is not clear yet. Administration of parathyroid hormone extract may help to distinguish between the two types. We report a case of a pseudohypoparathyroidism type Ib or II patient who had tetany, hypocalcemia and hyperphosphatemia with normal morphologic features.
Keyword
MeSH Terms
Figure
-

Fig. 1 The contour of patient's face. No gross abnormality.
Fig. 2 A. The contour of patient's hand. No gross abnormality. B. The contour of patient's hand. No gross abnormality.
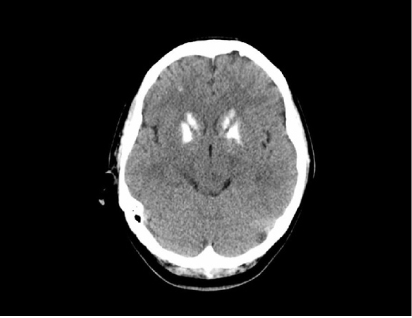
Fig. 3 Brain CT image. Symmetric high attenuation is noted in the basal ganglia and dentate nucleus suggesting calcification.
Fig. 4 Electroencephalography (EEG). EEG shows normal pattern.

Fig. 5 Both hand AP image. No gross bony abnormality.
Reference
-
1. Albright F, Burnett CH, Smith PH, Parson W. Pseudohypoparathyroidism: an example of the "Seabright-Bantam syndrome". Endocrinology. 1942. 30:922–932.2. Kang MH, Min YK, Chung YH, Hwang SD, Kim SY, Lee HK, Min HK. The variability of clinical and biochemical manifestation of pseudohypoparathyroidism. Korean J Int Med. 1985. 28:103–108.3. Ko BG, Hong SG, Jin SH, Park DC, Cho JT, Lee JK. A case of pseudohypoparathyroidism with atypical feature of Albright's hereditary osteodystrophy. Korean J Int Med. 1986. 31:130–135.4. Kang MI, Park YB, Lee YG, Yoo SJ, Son HS, Yoon KH, Hong KS, Lee KW, Son HY, Kang SK, Kim BS. Pseudohypoparathyroidism type Ia and type II. J Korean Endocr Soc. 1991. 6:170–178.5. Kim EY, Kim DK, Lee HJ, Jung EK, Park YB. A case of pseudohypoparathyroidism type II 1. J Korean Pediatr Soc. 1996. 39:1326–1330.6. Kim YS, Lee SH, Byun DI, Lee WK, Kim BH, Kim YH, Ko YS. A case of pseudohypoparathyroidism type I. J Korean Endocr Soc. 2006. 21:338–344.7. Spiegel AM, Gierschick P, Levine MA, Downs RW Jr. Clinical implications of guanine nucleotide-binding proteins as receptor-effector couplers. N Engl J Med. 1985. 312:26–33.8. Farfel Z, Brickman AS, Kaslow HR, Brothers VM, Bourne HR. Defect of receptor-cyclase coupling protein in pseudohypoparathyroidism. N Engl J Med. 1980. 303:237–242.9. Levine MA, Jap TS, Mauseth RS, Downs RW, Spiegel AM. Activity of the stimulatory guanine nucleotide-binding protein is reduced in erythrocytes from patients with pseudohypoparathyroidism and pseudopseudohypoparathyroidism: biochemical, endocrine, and genetic analysis of Albright's hereditary osteodystrophy in six kindreds. J Clin Endocrinol Metab. 1986. 62:497–502.10. Farfel Z, Bourne HR. Deficient activity of receptor-cyclase coupling protein in platelets of patients with pseudohypoparathyroidism. J Clin Endocrinol Metab. 1980. 51:1202–1204.11. Bourne HR, Kaslow HR, Brickman AS, Farfel Z. Fibroblast defect in pseudohypoparathyroidism, type I: reduced activity of receptor-cyclase coupling protein. J Clin Endocrinol Metab. 1981. 53:636–640.12. Farfel Z, Abood ME, Brickman AS, Bourne HR. Deficient activity of receptor-cyclase coupling protein is transformed lymphoblasts of patients with pseudohypoparathyroidism, type I. J Clin Endocrinol Metab. 1982. 55:113–117.13. Farfel Z, Friedman E. Mental deficiency in pseudohypoparathyroidism type I is associated with Ns-protein deficiency. Ann Intern Med. 1986. 105:197–199.14. Barett D, Breslau NA, Wax MB, Molinoff PB, Downs RW Jr. New form of pseudohypoparathyroidism with abnormal catalytic adenylate cyclase. Am J Physiol. 1989. 257:E277–E283.15. Linglart A, Carel JC, Garabedian M, Le T, Mallet E, Kottler ML. GNAS1 lesions in pseudohypoparathyroidism Ia and Ic: genotype phenotype relationship and evidence of the maternal transmission of the hormonal resistance. J Clin Endocrinol Metab. 2002. 87:189–197.16. Drezner M, Neelon FA, Lebovitz HE. Pseudohypoparathyroidism type II: a possible defect in the reception of the cyclic AMP signal. N Engl J Med. 1973. 289:1056–1060.17. Fukumoto S, Namba N, Ozono K, Yamauchi M, Sugimoto T, Michigami T, Tanaka H, Inoue D, Minagawa M, Endo I, Matsumoto T. Causes and differential diagnosis of hypocalcemia--recommendation proposed by expert panel supported by Ministry of Health, Labour and Welfare, Japan. Endocr J. 2008. 55:787–794.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Osteoma cutis in Albright's Hereditary Osteodystrophy
- Osteoma Cutis as the Presenting Feature of Albright Hereditary Osteodystrophy Associated with Pseudopseudohypoparathyroidism
- A Case of Pseudohypoparathyroidism in a Premature Infant
- A Case of Osteoma Cutis, a Diagnostic Clue for Albright's Hereditary Osteodystrophy
- A Case of Pseudohypoparathyroidism Worsened by Rhabdomyolysis
