J Clin Neurol.
2011 Mar;7(1):50-52. 10.3988/jcn.2011.7.1.50.
Atypical Presentation of Orbital Pseudotumor with Visual Loss as an Initial Manifestation
- Affiliations
-
- 1Department of Neurology, Haydarpasa Numune Education and Research Hospital, Istanbul, Turkey.
- 2Department of Neurosurgery, Goztepe Education and Research Hospital, Istanbul, Turkey. drnacibalak@yahoo.com
- KMID: 1452575
- DOI: http://doi.org/10.3988/jcn.2011.7.1.50
Abstract
- BACKGROUND
An orbital pseudotumor typically presents with periorbital pain, cranial nerve palsies and proptosis. Although visual deterioration is not unexpected in this pathology, its presentation solely with visual loss is unusual.
CASE REPORT
In this short report, we summarize a case of orbital pseudotumor which presented solely with a decrease in visual acuity, and discuss the clinical and radiological findings.
CONCLUSIONS
This atypical presentation likely resulted from the orbital pseudotumor originating in the optic foramen, leaving the neurovascular structures of the superior orbital fissure untouched initially. In the early clinical period, an orbital pseudotumor may manifest itself solely by visual loss. It should therefore be included in the differential diagnosis of visual pathologies-even in the absence of orbital pain and symptoms related to ocular movements.
Keyword
MeSH Terms
Figure
-
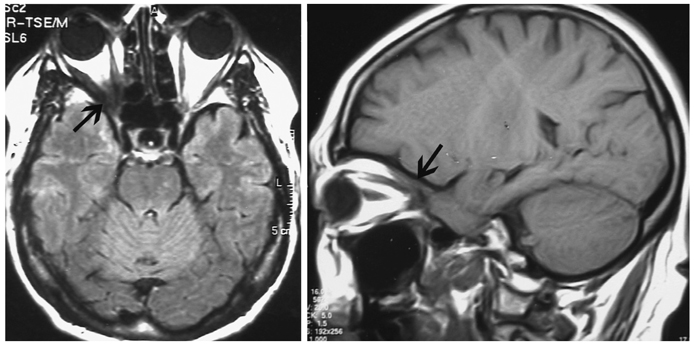
Fig. 1 Cranial axial FLAIR and sagittal T1-weighted MRI scans show a small mass lesion in the right optic foramen. The lesion is iso-intense. FLAIR: fluid attenuated inversion recovery.
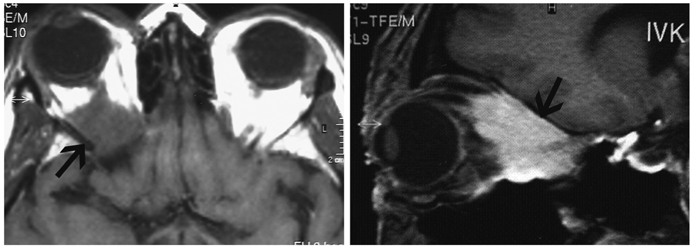
Fig. 2 T1-weighted axial and sagittal orbital MRI scans, without and with contrast media respectively, show a significantly large retrobulbar orbital lesion. The lesion is iso-intense and strongly enhanced after contrast injection.
Reference
-
1. Hogan RN. Levin LA, Arnold AC, editors. Orbital inflammation and infection. Neuro-ophthalmology the Practical Guide. 2005. New York: Thieme Medical Publishers Inc;356–386.2. Mahr MA, Salomao DR, Garrity JA. Inflammatory orbital pseudotumor with extension beyond the orbit. Am J Ophthalmol. 2004. 138:396–400.
Article3. Wasmeier C, Pfadenhauer K, Rösler A. Idiopathic inflammatory pseudotumor of the orbit and Tolosa-Hunt syndrome--are they the same disease? J Neurol. 2002. 249:1237–1241.
Article4. Birch-Hirschfeld A. Zur Diagnostik und Pathologie der Orbitaltumoren. Ber Dtsch Ophthal Ges. 1905. 32:127–135.5. Abramovitz JN, Kasdon DL, Sutula F, Post KD, Chong FK. Sclerosing orbital pseudotumor. Neurosurgery. 1983. 12:463–468.
Article6. Reittner P, Riepl T, Goritschnig T, Preidler KW, Koele W, Szolar DH. Bilateral orbital pseudotumour due to Ormond's disease: MR imaging and CT findings. Neuroradiology. 2002. 44:272–274.
Article7. Nugent RA, Rootman J, Robertson WD, Lapointe JS, Harrison PB. Acute orbital pseudotumors: classification and CT features. AJR Am J Roentgenol. 1981. 137:957–962.
Article8. McNicholas MM, Power WJ, Griffin JF. Idiopathic inflammatory pseudotumour of the orbit: CT features correlated with clinical outcome. Clin Radiol. 1991. 44:3–7.
Article9. Hurwitz BS, Citrin CM. Use of computerized axial tomography (CAT scan) in evaluating therapy of orbital pseudotumor. Ann Ophthalmol. 1979. 11:217–221.10. Turkoglu R, Balak N, Tireli H. Surgery With Cavernous Sinus Syndrome. A Clinical Study and Review of the Tolosa-Hunt Syndrome. Neurosurg Q. 2008. 18:230–238.
