J Clin Neurol.
2011 Mar;7(1):34-39. 10.3988/jcn.2011.7.1.34.
Visual Evoked Potentials in Guillain-Barre Syndrome
- Affiliations
-
- 1Department of Neurology, Ondokuz Mayis University School of Medicine, Samsun, Turkey. ligungor@omu.edu.tr
- 2Department of Ophthalmology, Ondokuz Mayis University School of Medicine, Samsun, Turkey.
- KMID: 1452571
- DOI: http://doi.org/10.3988/jcn.2011.7.1.34
Abstract
- BACKGROUND AND PURPOSE
Guillain-Barre syndrome (GBS) is an acute demyelinating polyneuropathy with various clinical features. Optic neuritis occurs in rare cases. In this study we determined the incidence and patterns of visual evoked potential (VEP) abnormality in GBS in association with ophthalmologic findings.
METHODS
Thirty-two patients with a diagnosis of GBS were included in the study. The correlation between pathologic VEPs and categories of neurologic deficit and electrophysiological findings were examined statistically.
RESULTS
The patients ranged in age from 19 to 77 years. Five cases (16%) had abnormal VEPs. All five of these patients exhibited increased P100 latency differences between the two eyes. Other abnormalities were prolonged p100 latency, increased interocular amplitude difference, and distorted p100 configuration. Pathologic signs on ophthalmologic examination were observed in 80% of patients with abnormal VEPs. VEP abnormality was never present in pure axonal forms. There was no significant correlation between pathologic VEP and cerebrospinal fluid protein level or categories of neurologic deficits.
CONCLUSIONS
Involvement of the optic pathways is not a frequent finding in GBS. When present it is always asymmetric and generally accompanied with pathologic findings on ophthalmologic examination. VEPs may be abnormal in different clinical variants of GBS, and especially in demyelinating forms.
MeSH Terms
Figure
-
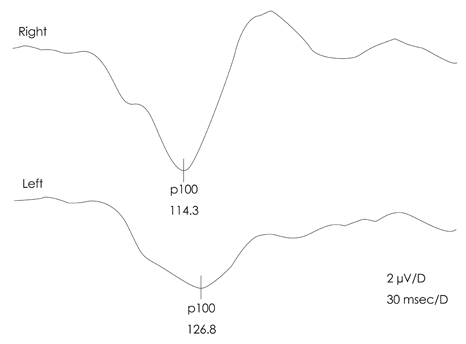
Fig. 1 Pathologic VEP of a patient with GBS (no. 3). The P100 latency is elongated on the left side, and has a low amplitude (lower trace), while it is normal on the right side (upper trace).
Reference
-
1. Hughes RA, Hadden RD, Gregson NA, Smith KJ. Pathogenesis of Guillain-Barré syndrome. J Neuroimmunol. 1999. 100:74–97.
Article2. Hartung HP, Kieseier BC, Kiefer R. Progress in Guillain-Barré syndrome. Curr Opin Neurol. 2001. 14:597–604.
Article3. Igarashi O, Fujioka T, Kishi M, Normoto N, Iwasaki Y, Kurihara T. Guillain-Barré syndrome with optic neuritis and cytomegalovirus infection. J Peripher Nerv Syst. 2005. 10:340–341.
Article4. Durand MC, Goulon-Goéau C, Schweitzer A, Chéliout-Héraut F, Raphael JC, Gajdos P. [Electrophysiologic study of 10 cases of Miller Fisher syndrome]. Rev Neurol (Paris). 2001. 157:72–79.5. Zgorzalewicz M, Zielińska M, Kilarski D. [Brain stem auditory and visual evoked potentials in children and adolescents with Guillain-Barré syndrome]. Neurol Neurochir Pol. 2004. 38:S31–S37.6. Wong V. A neurophysiological study in children with Miller Fisher syndrome and Guillain-Barre syndrome. Brain Dev. 1997. 19:197–204.
Article7. Topçu M, Ergin M, Nurlu G, Renda Y, Kanra G, Seçmeer G. Evoked potentials in Guillain-Barré syndrome. Turk J Pediatr. 1993. 35:79–85.8. Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barré syndrome. Ann Neurol. 1990. 27:Suppl. S21–S24.
Article9. Research criteria for diagnosis of chronic inflammatory demyelinating polyneuropathy (CIDP). Report from an Ad Hoc Subcommittee of the American Academy of Neurology AIDS Task Force. Neurology. 1991. 41:617–618.10. Van der Meché FG, Van Doorn PA, Meulstee J, Jennekens FG. GBS-consensus group of the Dutch Neuromuscular Research Support Centre. Diagnostic and classification criteria for the Guillain-Barré syndrome. Eur Neurol. 2001. 45:133–139.
Article11. Hughes JR, Stone JL, Fino JJ, Hart LA. Usefulness of different stimuli in visual evoked potentials. Neurology. 1987. 37:656–662.
Article12. Delisa JA. Delisa JA, Lee HJ, Baran EM, Lai K, Spielholz N, Mackenzie K, editors. Auditory and visual evoked potentials. Manual of nerve conduction velocity and clinical neurophysiology. 1994. Philadelphia: Lippincott Williams and Wilkins;294–304.13. Morley JB, Reynolds EH. Papilloedema and the Landry-Guillain-Barré syndrome. Case reports and a review. Brain. 1966. 89:205–222.14. Behan PO, Lessell S, Roche M. Optic neuritis in the Landry-Guillain-Barré-Strohl syndrome. Br J Ophthalmol. 1976. 60:58–59.15. Mori M, Kuwabara S, Fukutake T, Yuki N, Hattori T. Clinical features and prognosis of Miller Fisher syndrome. Neurology. 2001. 56:1104–1106.
Article16. Lüke C, Dohmen C, Dietlein TS, Brunner R, Lüke M, Krieglstein GK. [High-dose intravenous immunoglobulins for treatment of optic neuritis in Guillain-Barré syndrome]. Klin Monbl Augenheilkd. 2007. 224:932–934.17. Nadkarni N, Lisak RP. Guillain-Barré syndrome (GBS) with bilateral optic neuritis and central white matter disease. Neurology. 1993. 43:842–843.
Article18. Pfausler B, Engelhardt K, Kampfl A, Spiss H, Taferner E, Schmutzhard E. Post-infectious central and peripheral nervous system diseases complicating Mycoplasma pneumoniae infection. Report of three cases and review of the literature. Eur J Neurol. 2002. 9:93–96.
Article19. Caccavale A, Mignemi L. Acute onset of a bilateral areflexical mydriasis in Miller-Fisher syndrome: a rare neuro-ophthalmologic disease. J Neuroophthalmol. 2000. 20:61–62.
Article20. Hayashi Y, Fukuhara N, Yuki N. [Atypical Guillain-Barré syndrome associated with ophthalmoplegia and visual impairment following herpes simplex virus type 1 infection]. Rinsho Shinkeigaku. 1994. 34:724–726.21. Robbins MS, Roth S, Swerdlow ML, Bieri P, Herskovitz S. Optic neuritis and palatal dysarthria as presenting features of post-infectious GQ1b antibody syndrome. Clin Neurol Neurosurg. 2009. 111:465–466.
Article22. Stevenson VL, Ferguson SM, Bain PG. Bickerstaff's brainstem encephalitis, Miller Fisher syndrome and Guillain-Barre syndrome overlap with negative anti-GQ1b antibodies. Eur J Neurol. 2003. 10:187.
Article23. Lolekha P, Phanthumchinda K. Optic neuritis in a patient with Miller-Fisher syndrome. J Med Assoc Thai. 2008. 91:1909–1913.24. Chan JW. Optic neuritis in anti-GQ1b positive recurrent Miller Fisher syndrome. Br J Ophthalmol. 2003. 87:1185–1186.
Article25. Ginestal RC, Plaza JF, Callejo JM, Rodríguez-Espinosa N, Fernández-Ruiz LC, Masjuán J. Bilateral optic neuritis and Guillain-Barré syndrome following an acute Mycoplasma pneumoniae infection. J Neurol. 2004. 251:767–768.
Article26. Colding-Jørgensen E, Vissing J. Visual impairment in anti-GQ1b positive Miller Fisher syndrome. Acta Neurol Scand. 2001. 103:259–260.
Article27. Ropper AH, Chiappa KH. Evoked potentials in Guillain-Barré syndrome. Neurology. 1986. 36:587–590.28. An JY, Yoon B, Kim JS, Song IU, Lee KS, Kim YI. Guillain-Barré syndrome with optic neuritis and a focal lesion in the central white matter following Epstein-Barr virus infection. Intern Med. 2008. 47:1539–1542.
Article29. Ouhabi H, Bourazza A, Rouimi A, Boutaleb N, Mosseddaq R. [Bilateral optic neuritis and ponto-mesencephalic involvement shown by MRI in Miller-Fisher syndrome]. Rev Neurol (Paris). 1998. 154:780–782.30. Pakalnis A, Drake ME Jr, Barohn RJ, Chakeres DW, Mendell JR. Evoked potentials in chronic inflammatory demyelinating polyneuropathy. Arch Neurol. 1988. 45:1014–1016.
Article31. Stojkovic T, de Seze J, Hurtevent JF, Arndt C, Beaume A, Hache JC, et al. Visual evoked potentials study in chronic idiopathic inflammatory demyelinating polyneuropathy. Clin Neurophysiol. 2000. 111:2285–2291.
Article32. Uncini A, Gallucci M, Lugaresi A, Porrini AM, Onofrj M, Gambi D. CNS involvement in chronic inflammatory demyelinating polyneuropathy: an electrophysiological and MRI study. Electromyogr Clin Neurophysiol. 1991. 31:365–371.33. Carvalho AA, Galvão MD, Rocha MS, Piccolo AC, Maia SC. [Miller fisher syndrome and optic neuritis: case report]. Arq Neuropsiquiatr. 2000. 58:1115–1117.34. Cordonnier M, Caspers-Velu LE, Jacquemin C, van Nechel C, Tombroff M. Bilateral optic neuropathy and white dot syndrome following a mycoplasmal infection. Br J Ophthalmol. 1993. 77:673–676.
Article35. Fuller GN, Jacobs JM, Lewis PD, Lane RJ. Pseudoaxonal Guillain-Barré syndrome: severe demyelination mimicking axonopathy. A case with pupillary involvement. J Neurol Neurosurg Psychiatry. 1992. 55:1079–1083.
Article36. Hatanaka K, Nakasato N, Seki K, Kanno A, Mizoi K, Yoshimoto T. Striate cortical generators of the N75, P100 and N145 components localized by pattern reversal visual evoked magnetic fields. Tohoku J Exp Med. 1997. 182:9–14.
Article37. Bajaj NP, Rose P, Clifford-Jones R, Hughes PJ. Acute transverse myelitis and Guillain-Barré overlap syndrome with serological evidence for mumps viraemia. Acta Neurol Scand. 2001. 104:239–242.
Article38. Milla E, Zografos L, Piguet B. Bilateral optic papillitis following mycoplasma pneumoniae pneumonia. Ophthalmologica. 1998. 212:344–346.
Article39. Toshniwal P. Demyelinating optic neuropathy with Miller-Fisher syndrome. The case for overlap syndromes with central and peripheral demyelination. J Neurol. 1987. 234:353–358.
Article40. Yoshino H, Maeda Y, King M, Cartwright MJ, Richards DW, Ariga T, et al. Sulfated glucuronyl glycolipids and gangliosides in the optic nerve of humans. Neurology. 1993. 43:408–411.
Article41. Chiba A, Kusunoki S, Obata H, Machinami R, Kanazawa I. Ganglioside composition of the human cranial nerves, with special reference to the pathophysiology of Miller Fisher syndrome. Brain Res. 1997. 745:32–36.
Article42. Sasaki Y, Takubo H, Arai T, Machida Y, Ikebe S, Yuki N, et al. [Atypical Fisher syndrome with optic nerve involvement]. No To Shinkei. 2001. 53:571–573.43. Li H, Yuan J. Miller Fisher syndrome: toward a more comprehensive understanding. Chin Med J (Engl). 2001. 114:235–239.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bickerstaff's Brainstem Encephalitis with Guillain-Barre Syndrome Presenting Optic Neuropathy and Seizure
- Guillain-Barre Syndrome Combined with Acute Cervical Myelopathy
- Guillain-Barre Syndrome Associated with Tsutsugamushi Disease
- Therapeutic effects of plasmapheresis in Guillian-Barre syndrome
- Guillain-Barre Syndrome Presenting With Bilateral Ptosis
