Amylase, lipase, and volume of drainage fluid in gastrectomy for the early detection of complications caused by pancreatic leakage
- Affiliations
-
- 1Department of Surgery, Kosin University College of Medicine, Busan, Korea.
- 2Department of Surgery, On Hospital, Kosin University College of Medicine, Busan, Korea.
- 3Department of Laboratory Medicine, Kosin University College of Medicine, Busan, Korea. terminom@hanmail.net
- KMID: 1445769
- DOI: http://doi.org/10.4174/jkss.2011.81.6.402
Abstract
- PURPOSE
Pancreatic leakage is a serious complication of gastrectomy due to stomach cancer. Therefore, we analyzed amylase and lipase concentrations in blood and drainage fluid, and evaluated the volume of drainage fluid to discern their usefulness as markers for the early detection of serious pancreatic leakage requiring reoperation after gastrectomy.
METHODS
From January 2001 to December 2007, we retrospectively analyzed data from 24,072 patient samples. We divided patients into two groups; 1) complications with pancreatic leakage (CG), and 2) no complications associated with pancreatic leakage (NCG). Values of amylase and lipase in the blood and drainage fluid, volume of the drainage fluid, and relationships among the volumes, amylase values, and lipase values in the drainage fluid were evaluated, respectively in the two groups.
RESULTS
The mean amylase values of CG were significantly higher than those of NCG in blood and drainage fluid (P < 0.05). For lipase, statistically significant differences were observed in drainage fluid (P < 0.05). The mean volume (standard deviation) of the drained fluid through the tube between CG (n = 22) and NCG (n = 236) on postoperative day 1 were 368.41 (266.25) and 299.26 (300.28), respectively. There were no statistically significant differences between the groups (P = 0.298). There was a correlation between the amylase and lipase values in the drainage fluid (r = 0.812, P = 0.000).
CONCLUSION
Among postoperative amylase and lipase values in blood and drainage fluid, and the volume of drainage fluid, the amylase in drainage fluid was better differentiated between CG and NCG than other markers. The volume of the drainage fluid did not differ significantly between groups.
MeSH Terms
Figure
-

Fig. 1 Receiver operating characteristic (ROC) of amylase and lipase in blood. ROC curve created to identify the cut-off value of amylase concentration. Figures in parentheses are sensitivity and specificity. The area under the ROC curve (AUC) is 0.731 and 0.535 for amylase and lipase, respectively.

Fig. 2 Receiver operating characteristic (ROC) of amylase and lipase in drainage fluid. ROC curve created to identify the cut-off value of amylase concentration. Figures in parentheses are sensitivity and specificity. The area under the ROC curve (AUC) is 0.797 and 0.735 for amylase and lipase, respectively. The AUC value was highest for amylase from the drainage fluid.
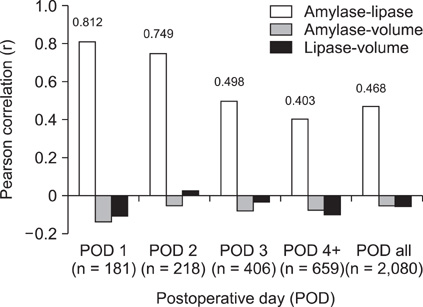
Fig. 3 Correlations among amylase, lipase, and volume in the drainage fluid by postoperative day. No significant correlation between the volume of drainage fluid and amylase or lipase concentrations was observed. POD, Postoperative day; POD 4+, From POD 4 to the rest POD; POD all, All postoperative days' data included.
Cited by 1 articles
-
Does international study group on pancreatic fistula (ISGPF) classification need modification after distal pancreatectomy?
In Geol Ho, Jae Keun Kim, Ho Kyoung Hwang, Jae Young Kim, Joon Seong Park, Dong Sup Yoon
Korean J Hepatobiliary Pancreat Surg. 2014;18(3):90-93. doi: 10.14701/kjhbps.2014.18.3.90.
Reference
-
1. Sano T, Sasako M, Katai H, Maruyama K. Amylase concentration of drainage fluid after total gastrectomy. Br J Surg. 1997. 84:1310–1312.2. Robertson CS, Chung SC, Woods SD, Griffin SM, Raimes SA, Lau JT, et al. A prospective randomized trial comparing R1 subtotal gastrectomy with R3 total gastrectomy for antral cancer. Ann Surg. 1994. 220:176–182.3. Bonenkamp JJ, Songun I, Hermans J, Sasako M, Welvaart K, Plukker JT, et al. Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet. 1995. 345:745–748.4. Sasako M, McCulloch P, Kinoshita T, Maruyama K. New method to evaluate the therapeutic value of lymph node dissection for gastric cancer. Br J Surg. 1995. 82:346–351.5. Tanaka K, Miyashiro I, Yano M, Kishi K, Motoori M, Seki Y, et al. Accumulation of excess visceral fat is a risk factor for pancreatic fistula formation after total gastrectomy. Ann Surg Oncol. 2009. 16:1520–1525.6. Hur H, Lim YS, Jeon HM, Kim W. Management of anastomotic leakage after gastrointestinal surgery using fluoroscopy-guided foley catheter. J Korean Surg Soc. 2010. 78:165–170.7. Nobuoka D, Gotohda N, Konishi M, Nakagohri T, Takahashi S, Kinoshita T. Prevention of postoperative pancreatic fistula after total gastrectomy. World J Surg. 2008. 32:2261–2266.8. Okabayashi T, Kobayashi M, Sugimoto T, Okamoto K, Matsuura K, Araki K. Postoperative pancreatic fistula following surgery for gastric and pancreatic neoplasm; is distal pancreaticosplenectomy truly safe? Hepatogastroenterology. 2005. 52:233–236.9. Oh ST, Kim WS, Kim BS. Changing patterns of pancreatic enzyme after distal gastrectomy and the effect of protease inhibitor treatment. J Korean Surg Soc. 1997. 52:846–851.10. Molinari E, Bassi C, Salvia R, Butturini G, Crippa S, Talamini G, et al. Amylase value in drains after pancreatic resection as predictive factor of postoperative pancreatic fistula: results of a prospective study in 137 patients. Ann Surg. 2007. 246:281–287.11. Yamaguchi M, Nakano H, Midorikawa T, Yoshizawa Y, Sanada Y, Kumada K. Prediction of pancreatic fistula by amylase levels of drainage fluid on the first day after pancreatectomy. Hepatogastroenterology. 2003. 50:1155–1158.12. Geokas MC, Rinderknecht H, Brodrick JW, Largman C. Studies on the ascites fluid of acute pancreatitis in man. Am J Dig Dis. 1978. 23:182–188.13. Smith RB 3rd, Warren WD, Rivard AA Jr, Amerson JR. Pancreatic ascites: diagnosis and management with particular reference to surgical technics. Ann Surg. 1973. 177:538–546.14. Barua RL, Villa F, Steigmann F. Massive ascites due to pancreatitis. Am J Dig Dis. 1962. 7:900–906.15. Geffroy Y, Colin R, Testart J, Bourreille J, Ledouarec P, Paillot B, et al. Massive ascites in pancreatitis. Review apropos of 10 personal cases. Sem Hop. 1975. 51:927–934.16. Dugernier T, Laterre PF, Reynaert MS. Ascites fluid in severe acute pancreatitis: from pathophysiology to therapy. Acta Gastroenterol Belg. 2000. 63:264–268.17. Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005. 138:8–13.18. Iwata N, Kodera Y, Eguchi T, Ohashi N, Nakayama G, Koike M, et al. Amylase concentration of the drainage fluid as a risk factor for intra-abdominal abscess following gastrectomy for gastric cancer. World J Surg. 2010. 34:1534–1539.19. Perryman RG, Hoerr SO. Observations on postoperative pancreatitis and postoperative elevation of the serum amylase. Am J Surg. 1954. 88:417–420.20. Singh LM, Okukubo F, James PM Jr, Salmon J, Howard JM. Further studies on postoperative pancreatitis. Arch Surg. 1965. 90:43–49.21. Harada K, Kitamura M, Ikenaga T. Isoenzyme study on postoperative transient hyperamylasemia. Am J Gastroenterol. 1974. 61:121–126.22. Keighley MR, Johnson AG, Stevens AE. Raised serum amylase after upper abdominal operation. Br J Surg. 1969. 56:424–427.23. Bardenheier JA, Kaminski DL, Willman VL. Pancreatitis after biliary tract surgery. Am J Surg. 1968. 116:773–776.24. Miller SF, Whitaker JR Jr, Snyder RD. Incidence of elevated serum amylase levels and pancreatitis after upper abdominal surgery. Am J Surg. 1973. 125:535–537.25. Grimes DA, Schulz KF. Uses and abuses of screening tests. Lancet. 2002. 359:881–884.26. Kawai M, Tani M, Terasawa H, Ina S, Hirono S, Nishioka R, et al. Early removal of prophylactic drains reduces the risk of intra-abdominal infections in patients with pancreatic head resection: prospective study for 104 consecutive patients. Ann Surg. 2006. 244:1–7.27. Tani M, Kawai M, Terasawa H, Ueno M, Hama T, Hirono S, et al. Complications with reconstruction procedures in pylorus-preserving pancreaticoduodenectomy. World J Surg. 2005. 29:881–884.28. Tani M, Onishi H, Kinoshita H, Kawai M, Ueno M, Hama T, et al. The evaluation of duct-to-mucosal pancreaticojejunostomy in pancreaticoduodenectomy. World J Surg. 2005. 29:76–79.29. Yeo CJ, Cameron JL, Lillemoe KD, Sohn TA, Campbell KA, Sauter PK, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg. 2002. 236:355–366.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Changing patterns of Pancreatic enzyme after Distal Gastrectomy and the Effect of Protease Inhibitor Treatment
- Evaluation of the Clinical Usefulness for Pancreatic Amylase in Acute Pancreatitis
- Pancreatic Pseudocyst after Endoscopic Ultrasound-Guided Fine Needle Aspiration of Pancreatic Mass
- Long Percutaneous Stent Insertion in Pancreatic Duct and Monitoring of Pancreaticojejunostomy Site Leakage in Periampullary Cancer Patients
- Approach to Hyperamylasemia and Hyperlipasemia
