Pathologic Fracture of Unicameral Bone Cyst
- Affiliations
-
- 1Department of Orthopedic Surgery, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. osd11@paik.ac.kr
- KMID: 1444790
- DOI: http://doi.org/10.5292/jkbjts.2011.17.2.58
Abstract
- PURPOSE
The purpose of this study is to observe unicameral bone cyst (UBC) outcome after the fracture has healed and if there is any identifiable prognostic factors.
MATERIALS AND METHODS
13 UBC patients with pathologic fracture from 2001 to 2010 were reviewed. The mean follow up were 26 months (3-90 months). There were 11 male and 2 female patients and the mean age of the patients were 10.2 years old (6-16 years). 9 involved proximal humerusand 2 involved humerus shaft and 1 involved proximal femur and 1 involved proximal tibia. The treatment of UBC fracture was conservative cast application to heal the fracture initially, and 1 patient was treated with primary auto bone graft and open reduction with internal fixation. 5 patients were treated with steroid injection during follow up period and 2 patients with auto bone graft. We analyzed the change of UBC during pathologic fracture healing period and prognostic factor about age, the size of UBC, the involvement of physis.
RESULTS
The mean duration of the fracture healing was 8.2 months. Complete healing were occurred at 4 patients (31%). No statiscal difference was checked with age about UBC healing (p=0.42). But, more larger size about UBC and more closer to physis, the healing was difficult (p=0.05, p=0.03).
CONCLUSION
While pathologic fracture of UBC was possibly healed, active treatment should be applied especially those cysts that involvescloser area of the physis or large size.
MeSH Terms
Figure
-
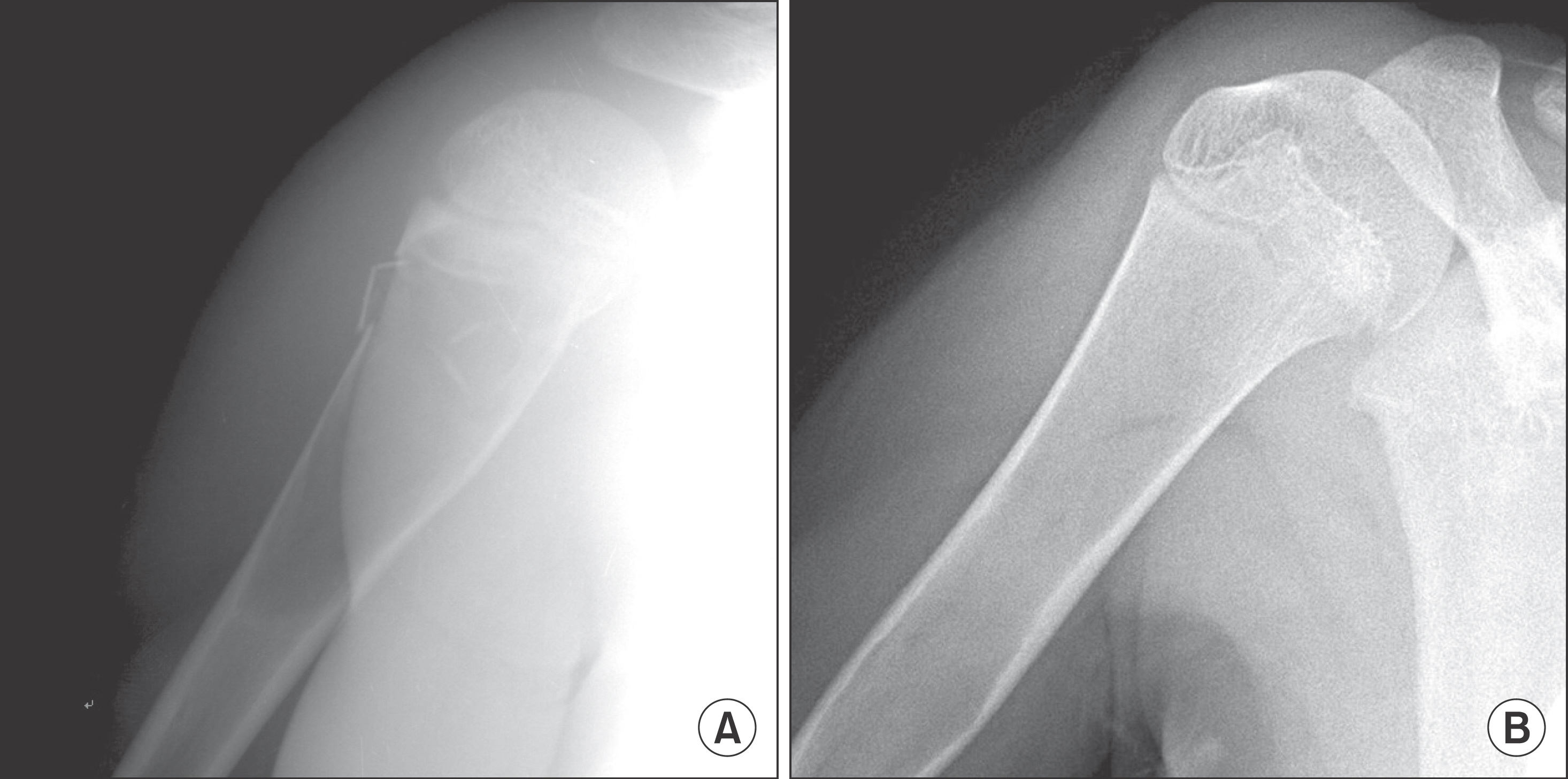
Figure 1. Completely healed case. (A) It was initial x-ray. (B) After treatment, the cystic lesion was completely resolved after duration 46 months.
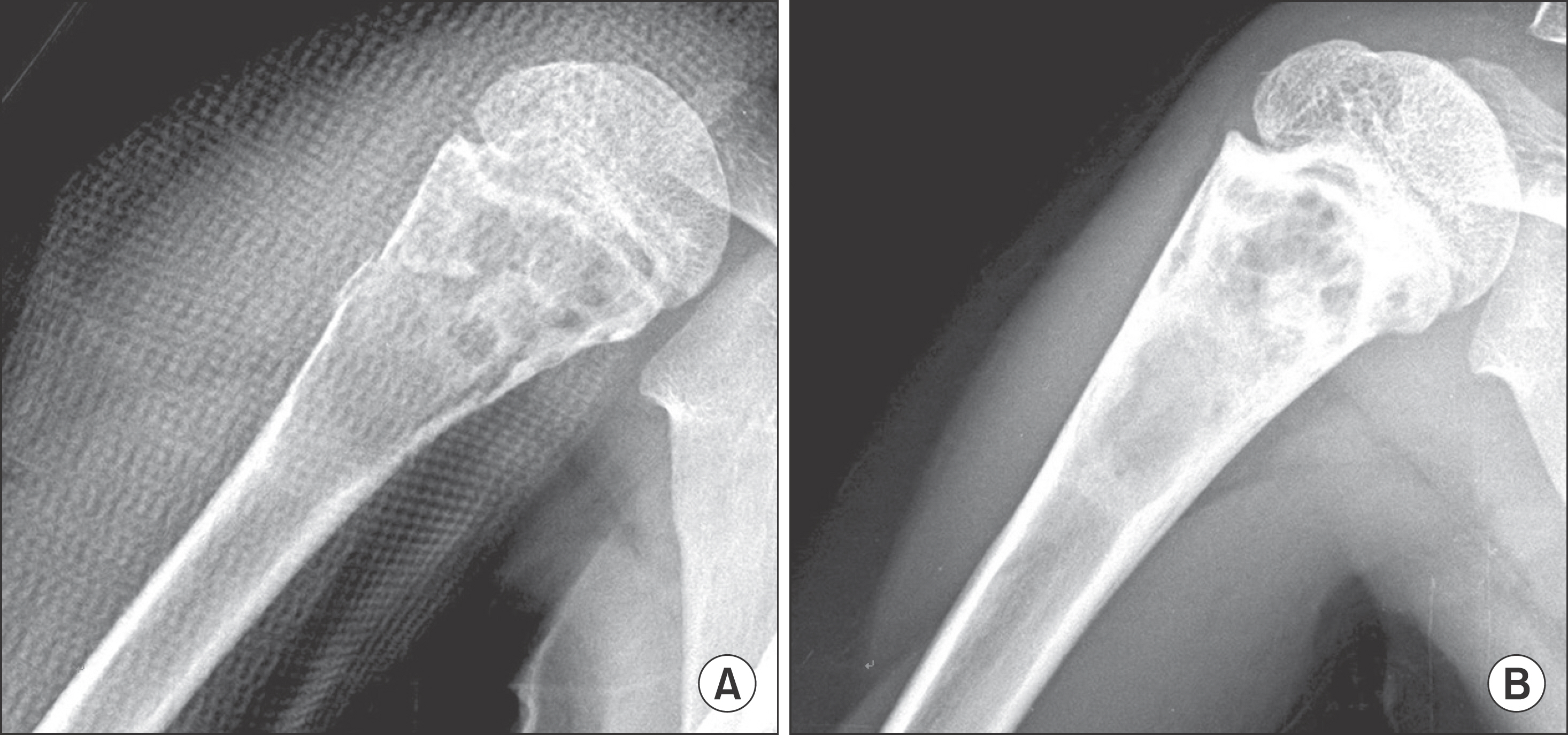
Figure 2. Partially healed case. (A) It was initial x-ray (B) After treatment, the cystic lesion was partially resolved after duration 4 months.

Figure 3. Recurrence case. (A) It was initial x-ray. (B) After treatment, the cystic lesion was partially resolved and fracture site was healed after duration 8 months. (C) But, after follow up 30 months, cystic lesion was recurred with another pathologic fracture.
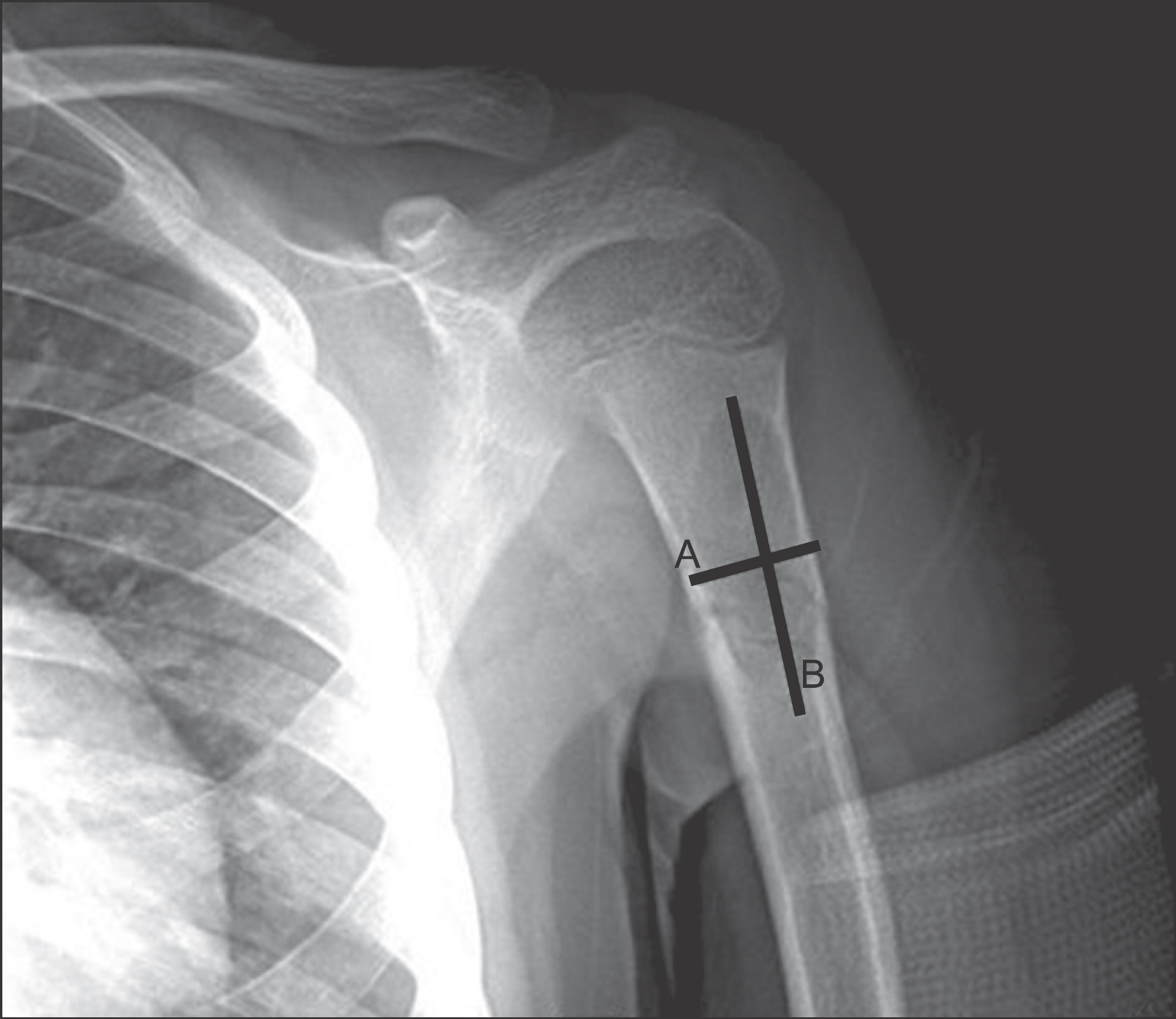
Figure 4. The measurement of cyst size. The maxium length was measured from medial cortex of cyst to lateral cortex (A). The maxium height was measured from upper margin of cyst to lower margin of cyst (B). Size=1/4×3.14×A×B.
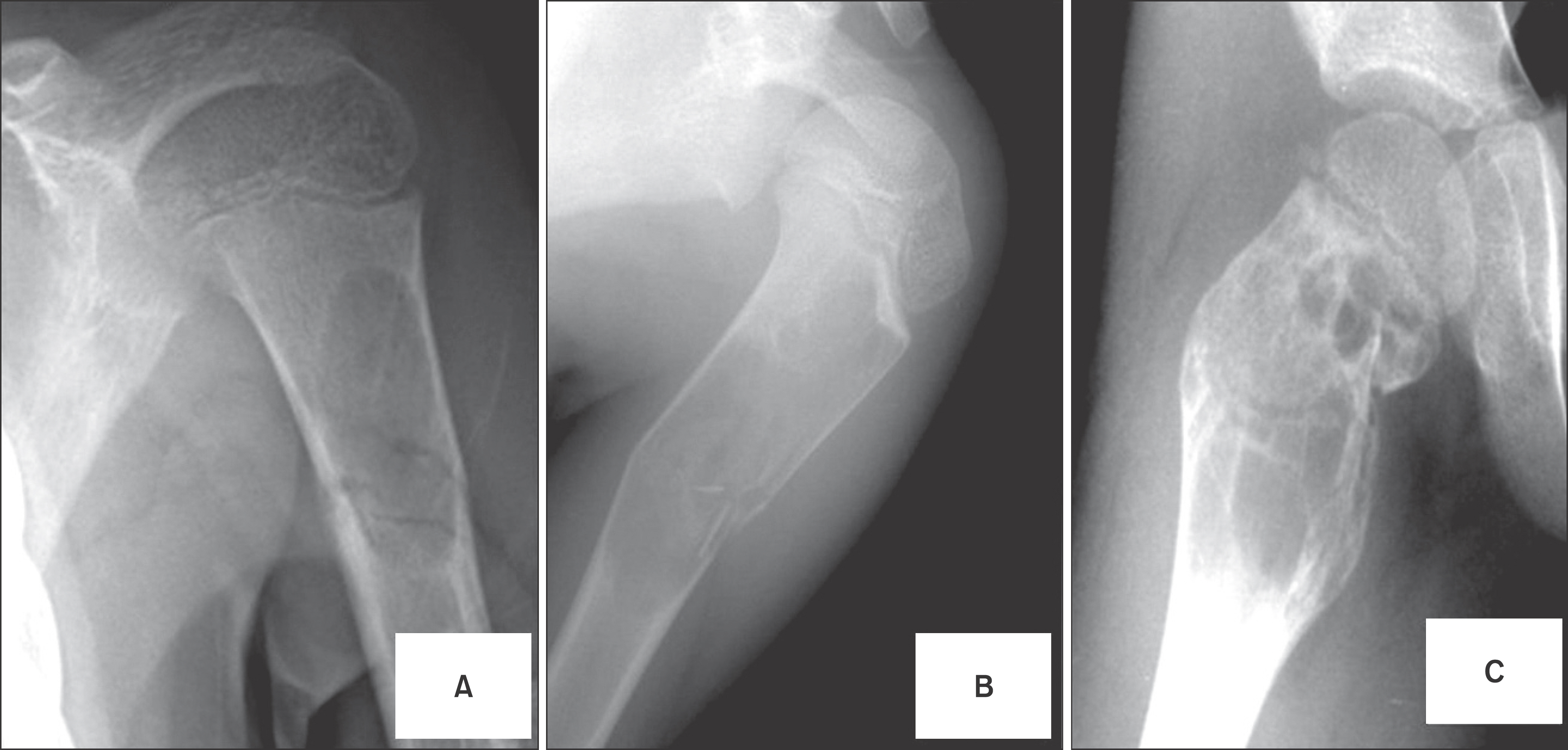
Figure 5. Involvement of physis. (A) Physis was not contacted (Grade I). (B) Physis was partially contacted (Grade II). (C) Physis was all contacted (Grade III).
Reference
-
References
1. Virchow R. Uber die Bildung von Knochenzysten. Berlin: Sit-zungb dAkad d Wissensch;1876. 369.2. Campanacci M, Capanna R, Picci P. Unicameral and aneurismal bone cysts. Clin Orthop. 1986; 204:25–36.3. Maski C, Susumu M, Satoru A, et al. The aetiology and treatment of simple bone cysts. Rhisho. Seiko. Geka. J Bone Joint Surg. 1983; 65B:633–7.4. Cohen J. Etiology of simple bone cyst. J Bone Joint Surg. 1970; 52A:1493–7.
Article6. Neer CS, Francis KC, Johnston AD, Kiernan HA Jr. Current concepts on the treatment of solitary unicameral bone cyst. Clin Orthop Relat Res. 1973; 97:40–51.
Article7. McKay DW, Nason SS. Treatment of unicameral bone cysts bysubtotal resection without grafts. J Bone Joint Surg Am. 1977; 59:515–9.8. Killian JT, Wilkinson L, White S, Brassard M. Treatment of unicameral bone cyst with demineralized bone matrix. J Pediatr Orthop. 1998; 18:621–4.
Article9. Lokiec F, Wientroub S. Simple bone cyst: etiology, classification, pathology, and treatment modalities. J Pediatr Orthop B. 1998; 7:262–73.10. Hahn SB, Kim NH, Park BM, Jeon CH. Comparison between treatment methods of simple bone cyst. J Korean Orthop Assoc. 1990; 25:941–9.11. Neer CS 2nd, Francis KC, Marcove RC, Terz J, Carbonara PN. Tretment of unicameral bone cyst. A follow-up study of one hundred seventy-five cases. J Bone Joint Surg Am. 1986; 48:731–45.12. Baker DM. Benign unicameral bone cyst. A study of fortyfive cases with long term follow up. Clin Orthop Relat Res. 1970; 71:140–51.13. Wilkins RM. Unicameral bone cysts. J Am Acad Orthop Surg. 2000; 8:217–24.
Article14. Makley JT, Joyce MJ. Unicameral bone cyst (simple bone cyst). Orthop Clin North Am. 1989; 20:407–15.15. Ahn JI, Park JS. Pathological fractures secondary to unicameral bone cysts. Int Orthop. 1994; 18:20–2.
Article16. Capannachia R, Dal Monte A, Gitelis S, Campanacci M. The natural history of unicameral bone cyst after steroid injuection. Clin Orthop. 1982; 166:204–11.17. Campanacci M, Capanna R, Picci P. Unicameral and aneurismal bone cysts. Clin Orthop Relat Res. 1986; 204:25–36.18. Oppenheim W, Galleno H. Operative treatment versus steroid injection in the management of unicameral bone cysts. J Pediatr Orthop. 1984; 4:1–7.
Article19. Moed BR, LaMont RL. Unicameral bone cyst complicated by growth retardation. J Bone Joint Surg Am. 1982; 64:1379–81.
Article20. Hecht AC, Gebhardt MC. Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr. 1998; 10:87–94.
Article21. Capanna R, Campanacci DA, Manfrini M. Unicameral and aneurysmal bone cysts. Orthop Clin North Am. 1996; 27:605–14.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Unicameral Bone Cyst with Fracture of Femoral Neck
- The Treatment of Unicameral Bone Cysts by Topical Injection of Methylprednisolone Acetate: Reaport of 4 Cases
- Unicameral Bone Cyst
- Recurrence of a Unicameral Bone Cyst in the Femoral Diaphysis
- The Treatment of Pathologic Troehanterie Fracture of the Femur by Solitary Bone Cyst in Children
