Thyroid Metastasis in Pyramidal Lobe from Renal Cell Carcinoma: A Case Report
- Affiliations
-
- 1Department of Radiology, Busan Paik Hospital, Inje University School of Medicine, Korea. dwultra@lycos.co.kr
- 2Department of Pathology, Busan Paik Hospital, Inje University School of Medicine, Korea.
- KMID: 1443502
- DOI: http://doi.org/10.3348/jksr.2011.64.6.537
Abstract
- Thyroid metastasis is rare. The most common primary malignancy of thyroid metastasis worldwide is known to be renal cell carcinoma, but the most common primary malignancy in South Korea is breast cancer. Many studies have reported that primary renal cell carcinoma is almost unilateral and thyroid metastasis from renal cell carcinoma is a nearly ipsilateral, single lesion. We report a case of pyramidal lobe metastasis from renal cell carcinoma.
Figure
-
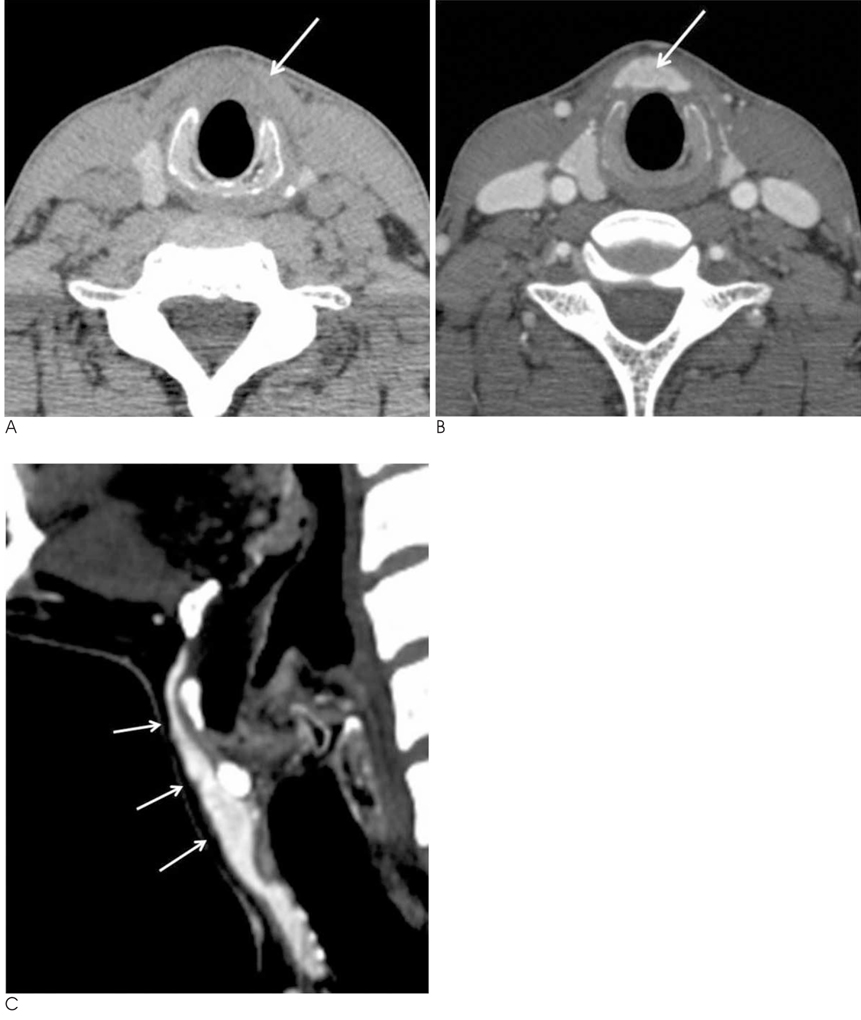
Fig. 1 The axial unenhanced (A), axial enhanced (B), and sagittal enhanced (C) CT scans show a diffuse enlargement, low attenuation, and well enhancement of pyramidal lobe (arrows) without a discrete nodule.
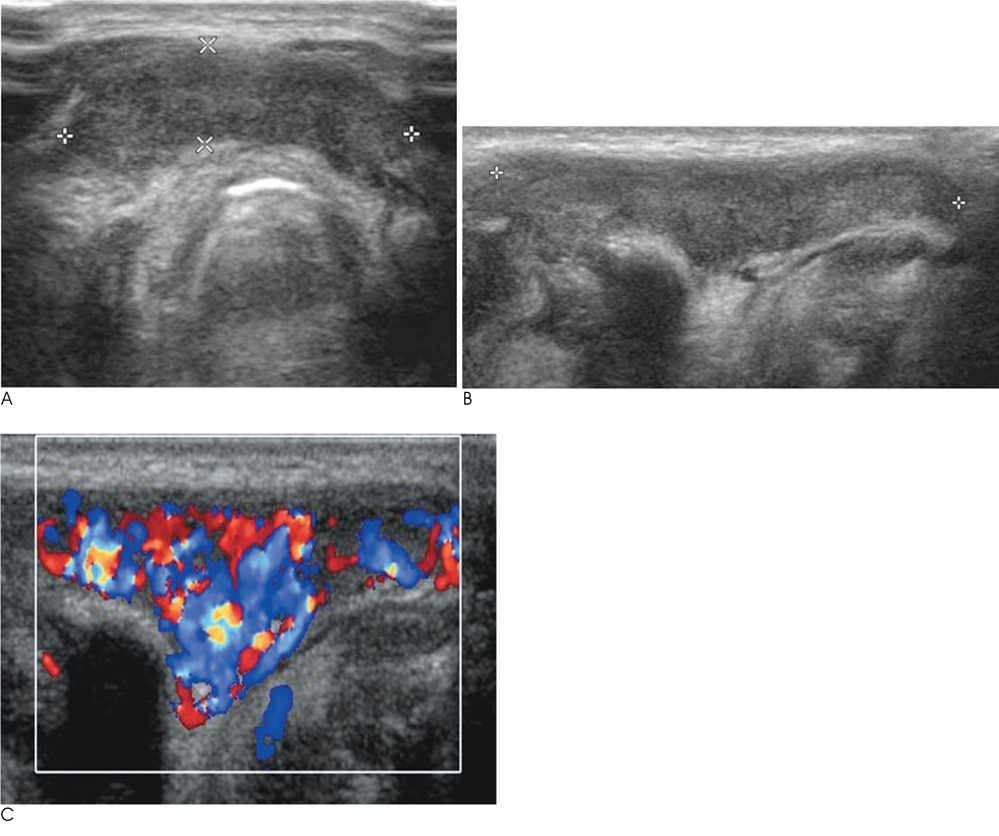
Fig. 2 A, B. The transverse and longitudinal sonograms show a diffuse enlargement and low echogenicity of pyramidal lobe. C. Longitudinal color Doppler sonogram shows moderately increased vascularity of pyramidal lobe.
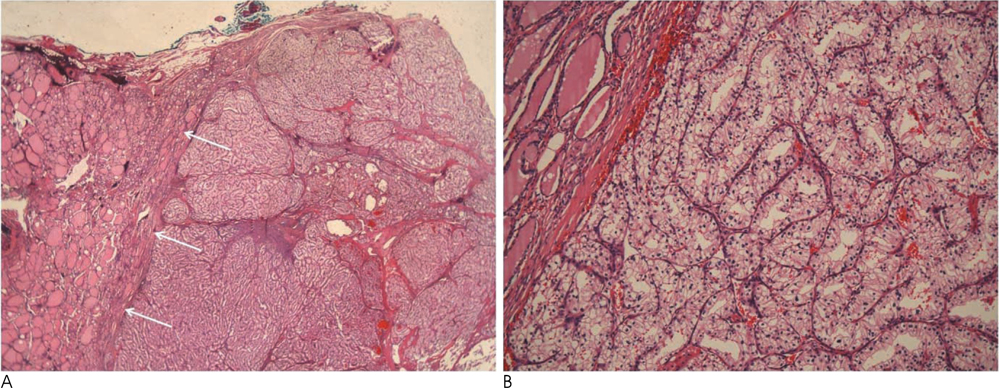
Fig. 3 A. A well-circumscribed mass is noted within thyroid parenchyma, and it shows lobular arrangement by thin fibrovascular septa (arrows) (H & E, ×10). B. The tumor shows compact, tubular or trabecular architecture separated by delicate vasculatures. The tumor cells show clear cytoplasms with distinct cell boundaries (H & E, ×200).
Reference
-
1. Rizzo M, Rossi RT, Bonaffini O, Scisca C, Sindoni A, Altavilla G, et al. Thyroid metastasis of clear cell renal carcinoma: report of a case. Diagn Cytopathol. 2009; 37:759–762.2. Papi G, Fadda G, Corsello SM, Corrado S, Rossi ED, Radighieri E, et al. Metastases to the thyroid gland: prevalence, clinicopathological aspects and prognosis: a 10-year experience. Clin Endocrinol (Oxf). 2007; 66:565–571.3. Takashima S, Takayama F, Wang JC, Saito A, Kawakami S, Kobayashi S, et al. Radiologic assessment of metastases to the thyroid gland. J Comput Assist Tomogr. 2000; 24:539–545.4. Kim AY, Park SB, Choi HS, Hwang JC. Isolated thyroid metastasis from renal cell carcinoma. J Ultrasound Med. 2007; 26:1799–1802.5. Kim TY, Kim WB, Gong GY, Hong SJ, Shong YK. Metastasis to the thyroid diagnosed by fine-needle aspiration biopsy. Clin Endocrinol (Oxf). 2005; 62:236–241.6. Won HS, Chung IH. Morphologic Variations of the Thyroid Gland in Korean Adults. Korean J Phys Anthropol. 2002; 15:119–125.7. Mortensen J, Woolner LB, Bennett WA. Secondary malignant tumors of the thyroid gland. Cancer. 1956; 9:306–309.8. Shimaoka K, Sokal JE, Pickren JW. Metastatic neoplasms in the thyroid gland. Pathologic and clinical findings. Cancer. 1962; 15:557–565.9. Dionigi G, Uccella S, Gandolfo M, Lai A, Bertocchi V, Rovera F, et al. Solitary intrathyroidal metastasis of renal clear cell carcinoma in a toxic substernal multinodular goiter. Thyroid Res. 2008; 1:6.10. Hoang JK, Lee WK, Lee M, Johnson D, Farrell S. US Features of thyroid malignancy: pearls and pitfalls. Radiographics. 2007; 27:847–860.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Papillary Carcinoma Arising from the Pyramidal Lobe of the Thyroid
- A Case Report of Metastatic Renal Cell Carcinoma to Thyroid
- Metastatic Clear Cell Renal Cell Carcinoma to the Thyroid Gland
- Two Cases of Renal Cell Carcinoma Metastatic to the Thyroid Gland
- Clinical characteristics of papillary thyroid carcinoma arising from the pyramidal lobe
