Partial Rupture of Semitendinosus Muscle at Satba (Thigh Band) Wearing Area in a Ssireum Athlete
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University Bucheon Hospital, Bucheon, Korea. kdmin@schmc.ac.kr
- 2Department of Orthopedic Surgery, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea.
- KMID: 1439993
- DOI: http://doi.org/10.4055/jkoa.2012.47.1.54
Abstract
- High load is concentrated on Satba wearing area of Ssireum athletes during the tournament. Muscular injuries in this area may seriously affect the athletic performance. We report a case of a 21-year-old Ssireum athlete who was experiencing pain in his left thigh (Satba wearing area) during a tournament due to the migrating mass effect of a partial ruptured semitendinosus muscle occurred approximately 6 months before. Herein is described the clinical results after surgical intervention with an added review of the relevant literature.
Keyword
Figure
-
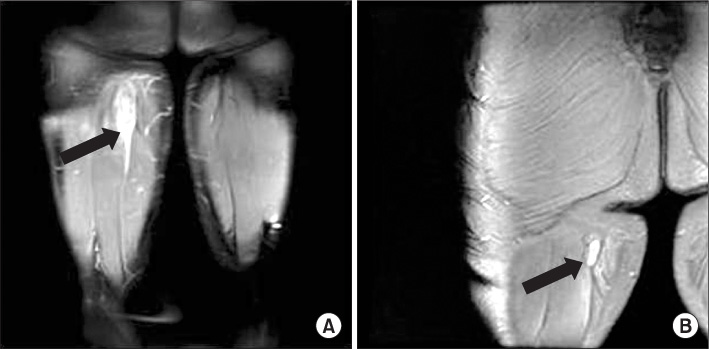
Figure 1 (A) Initial magnetic resonance imaging (MRI) finding shows ovoid mass-like lesion (arrow) at proximal semitendinosus muscle with high signal intensity on T2 coronal image surrounding soft tissue edema. (B) 6 months follow-up, MRI finding shows down sized ovoid mass having well defined margin (arrow) at the same site with high signal intensity on T2 coronal image.

Figure 2 (A) Torn end of semitendinosus muscle was exposed and excised between normal muscle and fibrous portion. (B) The muscle is extensively replaced by dilated vascular channels with thrombosis and mature adipose tissue (H&E stain, ×40).
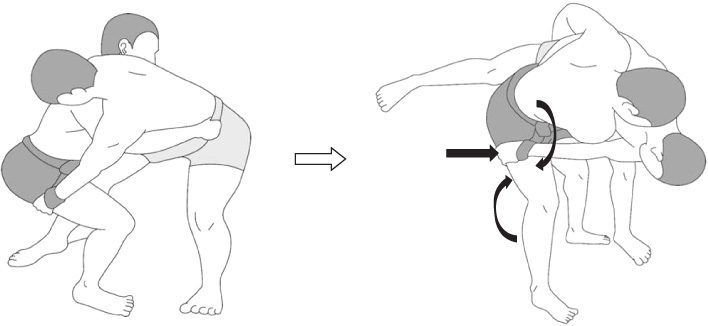
Figure 3 Schematic figure representing of the mechanism of injury. Note that eccentric contraction of hamstring muscle results from sudden knee extension and hip flexion of the pivoting lower extremity (curved arrow) in condition of adding excessive stress at Satba wearing area (straight arrow).
Reference
-
1. Chakravarthy J, Ramisetty N, Pimpalnerkar A, Mohtadi N. Surgical repair of complete proximal hamstring tendon ruptures in water skiers and bull riders: a report of four cases and review of the literature. Br J Sports Med. 2005. 39:569–572.
Article2. Lempainen L, Sarimo J, Heikkilä J, Mattila K, Orava S. Surgical treatment of partial tears of the proximal origin of the hamstring muscles. Br J Sports Med. 2006. 40:688–691.
Article3. Brucker PU, Imhoff AB. Functional assessment after acute and chronic complete ruptures of the proximal hamstring tendons. Knee Surg Sports Traumatol Arthrosc. 2005. 13:411–418.
Article4. Ishikawa K, Kai K, Mizuta H. Avulsion of the hamstring muscles from the ischial tuberosity. A report of two cases. Clin Orthop Relat Res. 1988. (232):153–155.5. Kujala UM, Orava S, Järvinen M. Hamstring injuries. Current trends in treatment and prevention. Sports Med. 1997. 23:397–404.6. Klingele KE, Sallay PI. Surgical repair of complete proximal hamstring tendon rupture. Am J Sports Med. 2002. 30:742–747.
Article7. Schache AG, Koulouris G, Kofoed W, Morris HG, Pandy MG. Rupture of the conjoint tendon at the proximal musculotendinous junction of the biceps femoris long head: a case report. Knee Surg Sports Traumatol Arthrosc. 2008. 16:797–802.
Article8. Rhee KJ, Kim YM, Hwang DS, et al. Resection of the proximal tendinous portion in avulsion of the semimembranosus tendon from the ischial tuberosity in an adult: a case report. J Korean Orthop Assoc. 2005. 40:617–621.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Semitendinosus Tendon Rupture in Non Athlete
- Muscle Infarction and Calcification of the Semitendinosus Tendon: A Case Report
- Rupture of The Adductor Longus Muscle of The Thigh: 5 Cases Report
- Chronic Tibialis Anterior Tendon Rupture Treated with Semitendinosus Autograft: A Report of Two Cases
- Reconstruction of Posterior Cruciate Ligament Using Semitendinosus Tendon (3 cases)
