Occult Invasive Lobular Carcinoma of Breast Detected by Stomach Metastasis: A Case Report
- Affiliations
-
- 1Department of Radiology, Bundang CHA General Hospital, CHA University College of Medicine, Seongnam, Korea. hhkkjung@hanmail.net
- KMID: 1439411
- DOI: http://doi.org/10.3348/jksr.2012.66.2.177
Abstract
- Gastric metastasis from primary breast cancer is a rare phenomenon that is more prevalent in the invasive lobular type of breast cancer. We describe a very rare case of occult invasive lobular cancer of the breast detected by the initial presentation of gastric metastasis in a patient without a history of breast cancer. A 18F-fluorodeoxyglucose positron-emission tomography/computed tomography (FDG PET/CT) which showed increased FDG uptake in the stomach, abdominal mesentery and the right breast, and played pivotal roles in the detection of occult primary breast cancer and a diagnosis of gastric metastasis as an ancillary method for obtaining histological results and immunohistochemical stains.
MeSH Terms
Figure
-

Fig. 1 Contrast-enhanced abdomen CT shows diffuse gastric wall thickening, from the esophago-gastric junction to the distal antrum (arrows), as well as a large amount of ascites.
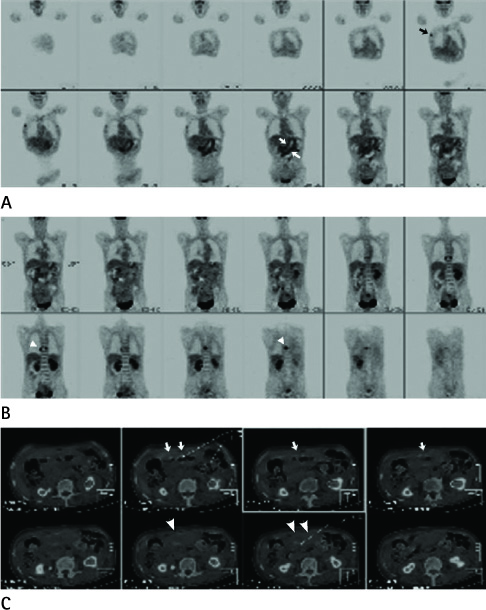
Fig. 2 A 57-year-old woman underwent FDG PET/CT to find a primary malignancy. A, B. Coronal images of the FDG-PET scan represent increased FDG uptake in the right breast (black arrow), stomach (white arrows), abdominal mesentery, and thoracic vertebral body (arrowheads). C. Axial images of PET-CT fusion show highlighted pathological FDG uptakes in the stomach (white arrows) and the abdominal mesenetery (arrowheads). Note.-FDG PET = 18F-fluorodeoxyglucose positron-emission tomography
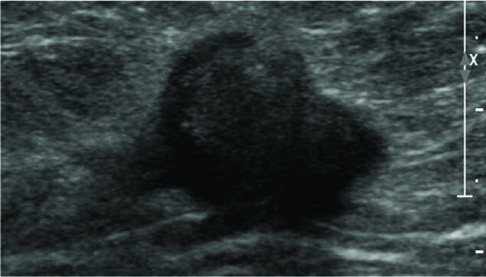
Fig. 3 Breast sonography shows irregular spiculated and hypoechoic nodules with maximum diameters measuring approximately 24 mm with a surrounding hyperechoic rim in the right upper outer breast.
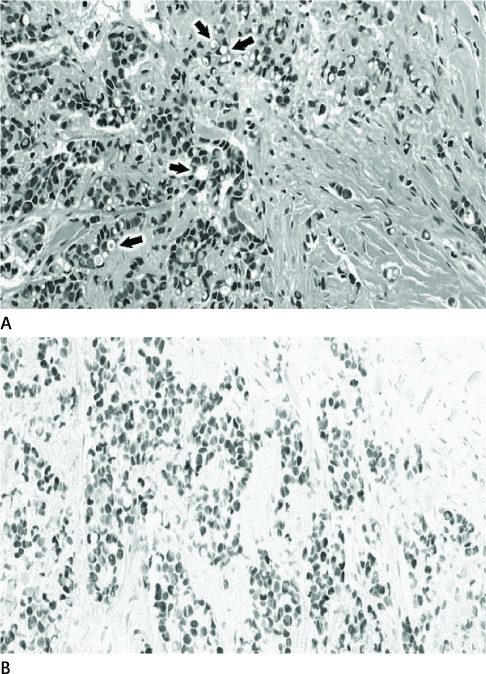
Fig. 4 A 57-year-old woman underwent sonography-guided breast core biopsy for the right breast nodule. A. Microscopic findings of breast core specimens reveal invasive lobular cancer cells with well-circumscribed signet ring cells as well as cytoplasmic vaculoes and eccentric nuclei (arrows) (H&E, × 100). B. Immunohistochemical staining of breast core specimens shows a positive estrogen receptor result (× 100).

Fig. 5 Endoscopic biopsy was performed for a huge depressed-ulcerative lesion at the lower body of the stomach in a 57-year-old woman. A. Microscopic observation of the endoscopic biopsy finds diffuse tumor infiltration (arrows) with signet cells (arrowheads) similar to the primary breast cancer in the gastric stroma with intact mucosa (H&E, × 100). B. Immunohistochemical staining of endoscopic stomach biopsy specimens represents in a positive estrogen receptor result (× 100).
Reference
-
1. Choi SH, Sheehan FR, Pickren JW. Metastatic involvement of the stomach by breast cancer. Cancer. 1964; 17:791–797.2. Taal BG, Peterse H, Boot H. Clinical presentation, endoscopic features, and treatment of gastric metastases from breast carcinoma. Cancer. 2000; 89:2214–2221.3. McLemore EC, Pockaj BA, Reynolds C, Gray RJ, Hernandez JL, Grant CS, et al. Breast cancer: presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol. 2005; 12:886–894.4. Ferri LE, Onerheim R, Emond C. Linitis plastica as the first indication of metastatic lobular carcinoma of the breast: case report and literature review. Can J Surg. 1999; 42:466–469.5. Elliott LA, Hall GD, Perren TJ, Spencer JA. Metastatic breast carcinoma involving the gastric antrum and duodenum: computed tomography appearances. Br J Radiol. 1995; 68:970–972.6. Pera M, Riera E, Lopez R, Viñolas N, Romagosa C, Miquel R. Metastatic carcinoma of the breast resembling early gastric carcinoma. Mayo Clin Proc. 2001; 76:205–207.7. Tremblay F, Jamison B, Meterissian S. Breast cancer masquerading as a primary gastric carcinoma. J Gastrointest Surg. 2002; 6:614–616.8. Ciulla A, Castronovo G, Tomasello G, Maiorana AM, Russo L, Daniele E, et al. Gastric metastases originating from occult breast lobular carcinoma: diagnostic and therapeutic problems. World J Surg Oncol. 2008; 6:78.9. Pectasides D, Psyrri A, Pliarchopoulou K, Floros T, Papaxoinis G, Skondra M, et al. Gastric metastases originating from breast cancer: report of 8 cases and review of the literature. Anticancer Res. 2009; 29:4759–4763.10. Kwee TC, Basu S, Cheng G, Alavi A. FDG PET/CT in carcinoma of unknown primary. Eur J Nucl Med Mol Imaging. 2010; 37:635–644.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nodular Metastatic Carcinoma from Invasive Lobular Breast Cancer
- Peritoneal and gastric metastasis from invasive lobular breast carcinoma: a case report
- Synchronously Diagnosed Gastric Metastasis from Invasive Lobular Breast Carcinoma, Mimicking Primary Gastric Carcinoma
- Invasive Lobular Carcinoma of the Breast Associated with Mixed Lobular and Ductal Carcinoma In Situ: A Case Report
- Abdominal Wall Metastasis from an Invasive Lobular Carcinoma of the Breast: A Case Report
