Clinical Outcome of Parosteal Osteosarcoma
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea Cancer Center Hospital, Seoul, Korea. dgjeon@kcch.re.kr
- KMID: 1431656
- DOI: http://doi.org/10.5292/jkbjts.2013.19.1.20
Abstract
- PURPOSE
The purpose of this study was to evaluate the oncologic outcomes of parosteal osteosarcoma (POS) and to ascertain the fates of patients after local recurrence (LR).
MATERIALS AND METHODS
The authors retrospectively reviewed 22 POS patients with an average follow-up of 114 months (range: 36-235 months). Seven of the 22 patients were referred after LR. There were 17 Stage IB and 5 Stage IIB (G2, 2; dedifferentiation, 3). Tumors were located in the femur (11) and in other locations (11). Initial surgical margins were wide in 10, marginal in 5, and intralesional in 7. Correlations between clinico-pathologic variables and LR and clinical courses after LR were evaluated.
RESULTS
The 10-year overall survival rate was 85.7%. Three (14%) patients developed distant metastasis and all of them succumbed to the disease. Nine (41%) patients developed LR. Tumor location, resection type, and surgical margin were found to be correlated with LR. At final follow-up, 7 of the 9 patients that experienced local failure achieved no evidence of disease.
CONCLUSION
A substantial risk of misdiagnosis exists, especially for POS in other than a femoral location. Recurrent tumor re-excision is possible in most cases; however, patients with an aggressive recurrence pattern deserve special attention.
Keyword
MeSH Terms
Figure
-
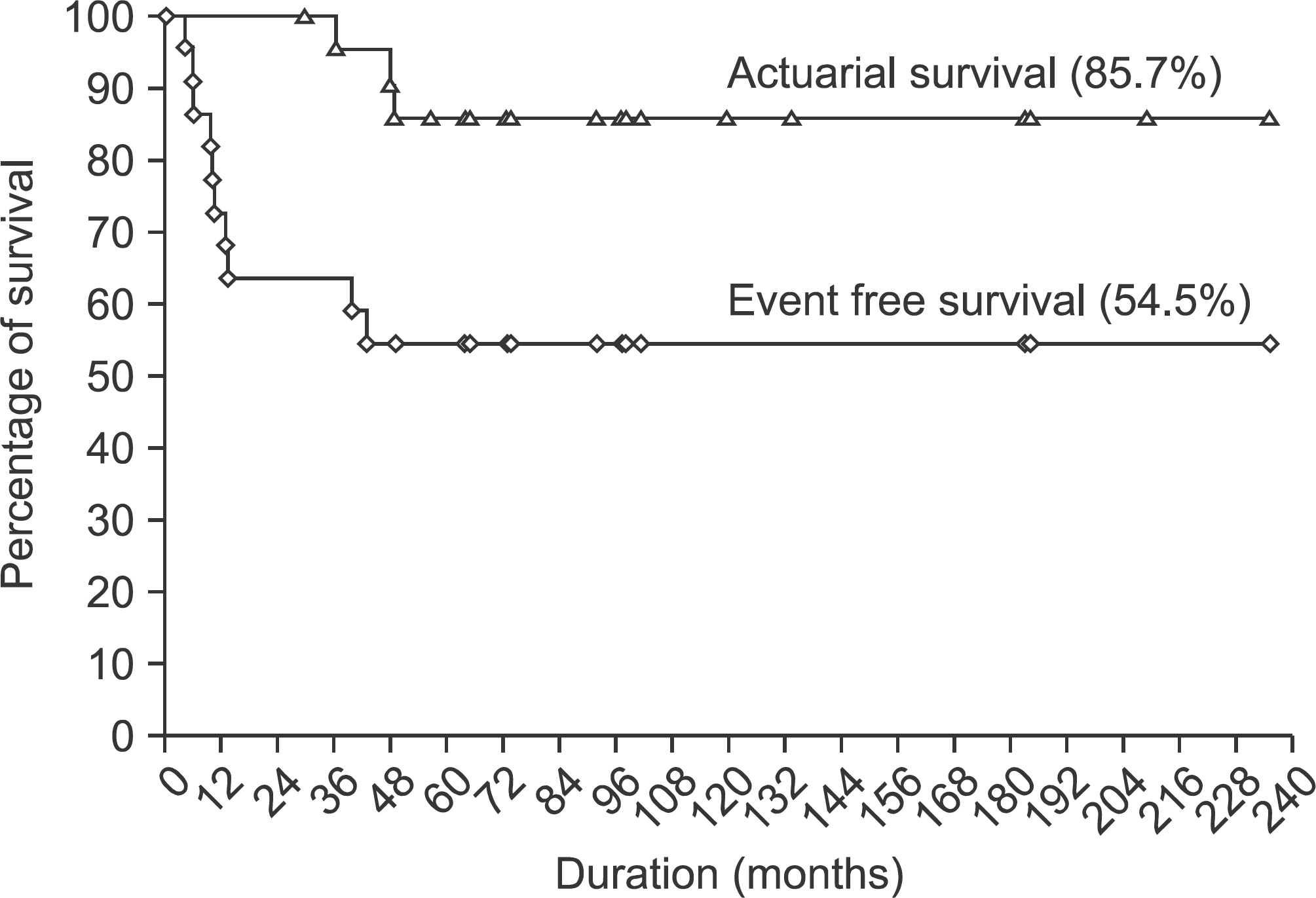
Figure 1. The 10-year overall and event free survival rates were determined using the Kaplan-Meier plot.

Figure 2. Patient 21 was a 37-year-old woman who was misdiagnosed as Nora's lesion. (A) Initial anteroposterior radiograph shows an ossified mass on the posterolateral aspect of humerus. (B) This anteroposterior radiograph was taken after 4 episodes of intralesional procedure at referral hospital. Note ill-defined calcified nodules which were located around proximal humerus. (C) The patient underwent segmental excision and reconstruction with recycled autograft. Local recurrence was noted on this anteroposterior radiograph taken after 3 month later. Concomitant metastasis was also identified.

Figure 3. A diagram shows the outcome in a meta-analysis of 21 locally recurrent patients. Nearly a half (10/21) of them underwent amputation to manage the local recurrence (LR, local recurrence; NED, no evidence of disease; DOD, dead of disease).
Reference
-
References
1. Raymond AK. Surface osteosarcoma. Clin Orthop Relat Res. 1991; 270:140–8.
Article2. Unni KK, Dahlin DC, Beabout JW. Periosteal osteogenic sarcoma. Cancer. 1976; 37:2476–85.
Article3. van der Heul RO, von Ronnen JR. Juxtacortical osteosarcoma. Diagnosis, differential diagnosis, treatment, and an analysis of eighty cases. J Bone Joint Surg Am. 1967; 49:415–39.4. Campanacci M, Picci P, Gherlinzoni F, Guerra A, Bertoni F, Neff JR. Parosteal osteosarcoma. J Bone Joint Surg Br. 1984; 66:313–21.
Article5. Han I, Oh JH, Na YG, Moon KC, Kim HS. Clinical outcome of parosteal osteosarcoma. J Surg Oncol. 2008; 97:146–9.
Article6. Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK. Parosteal osteosarcoma. A clinicopathological study. J Bone Joint Surg Am. 1994; 76:366–78.
Article7. Enneking WF, Springfield D, Gross M. The surgical treatment of parosteal osteosarcoma in long bones. J Bone Joint Surg Am. 1985; 67:125–35.
Article8. Kavanagh TG, Cannon SR, Pringle J, Stoker DJ, Kemp HB. Parosteal osteosarcoma. Treatment by wide resection and prosthetic replacement. J Bone Joint Surg Br. 1990; 72:959–65.
Article9. Ahuja SC, Villacin AB, Smith J, Bullough PG, Huvos AG, Marcove RC. Juxtacortical (parosteal) osteogenic sarcoma: histological grading and prognosis. J Bone Joint Surg Am. 1977; 59:632–47.10. Bertoni F, Bacchini P, Staals EL, Davidovitz P. Dedifferentiated parosteal osteosarcoma: the experience of the Rizzoli Institute. Cancer. 2005; 103:2373–82.
Article11. Jelinek JS, Murphey MD, Kransdorf MJ, Shmookler BM, Malawer MM, Hur RC. Parosteal osteosarcoma: value of MR imaging and CT in the prediction of histologic grade. Radiology. 1996; 201:837–42.
Article12. Wold LE, Unni KK, Beabout JW, Sim FH, Dahlin DC. Dedifferentiated parosteal osteosarcoma. J Bone Joint Surg Am. 1984; 66:53–9.
Article13. Ritschl P, Wurnig C, Lechner G, Roessner A. Parosteal osteosarcoma. 2–23-year follow-up of 33 patients. Acta Orthop Scand. 1991; 62:195–200.
Article14. Lewis VO, Gebhardt MC, Springfield DS. Parosteal osteosarcoma of the posterior aspect of the distal part of the femur. Oncological and functional results following a new resection technique. J Bone Joint Surg Am. 2000; 82A:1083–8.15. Temple HT, Scully SP, O'Keefe RJ, Katapurum S, Mankin HJ. Clinical outcome of 38 patients with juxtacortical osteosarcoma. Clin Orthop Relat Res. 2000; 373:208–17.
Article16. Sheth DS, Yasko AW, Raymond AK, et al. Conventional and dedifferentiated parosteal osteosarcoma. Diagnosis, treatment, and outcome. Cancer. 1996; 78:2136–45.
Article17. Grimer RJ, Sommerville S, Warnock D, et al. Management and outcome after local recurrence of osteosarcoma. Eur J Cancer. 2005; 41:578–83.
Article18. Luck JV Jr, Luck JV, Schwinn CP. Parosteal osteosarcoma: a treatment-oriented study. Clin Orthop Relat Res. 1980; 153:92–105.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Parosteal osteosarcoma of the scapula
- Osteosarcoma arising on the surface of long bones: a review of radiologic and histologic spectrum in 9 cases
- Parosteal Ossifying Lipoma of Femur: A Case Report
- Parosteal Lipoma of the Tibia: A Case Report
- Limb Salvage Surgery in a Rare Case of Recurrent Parosteal Osteosarcoma with Vascular Graft Thrombosis
