Traumatic Dislocation of the Hip with a Femoral Head Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, Sang-Gye Paik Hospital, College of Medicine, Inje University, Seoul, Korea. ybs58@paik.ac.kr
- KMID: 1425037
- DOI: http://doi.org/10.5371/hp.2013.25.1.57
Abstract
- PURPOSE
This study was designed in order to evaluate the clinical results and frequency of complications of patients who underwent surgical treatment for traumatic dislocation of the hip with a femoral head fracture.
MATERIALS AND METHODS
Eighteen cases of Thompson-Epstein type V femoral head fracture with dislocation of the hip from November 2002 to November 2011 were analyzed retrospectively. We divided the cases into two groups according to availability of closed reduction and reduction time, and analyzed the clinical results according to Epstein criteria and frequency of avascular necrosis of the femoral head and posttraumatic osteoarthritis.
RESULTS
Among all patients, the observed complications included three cases of avascular necrosis and one case of posttraumatic osteoarthritis. The data showed that 14 cases were available for closed reduction; otherwise, there were four cases of failure. Significant differences were observed in clinical results and frequency of complications. Results regarding reduction time showed that 10 cases took 6 hours, and the other eight cases took more than 6 hours. There were no differences in clinical results, but, better results were achieved with a reduction time in 6 hours. However, significant differences were observed in frequency of complications.
CONCLUSION
The availability of closed reduction would be an important factor for achievement of good clinical results in traumatic dislocation of the hip with a femoral head fracture. In order to obtain better clinical results, closed reduction should be performed as rapidly as possible.
Figure
-

Fig. 1 (A, B) A 23-year-old male sustained Pipkin type I fracture of hip. (C, D) Open reduction and internal fixation of femoral head with trochanter flip osteotomy was done. The radiograph and CT at postoperative 20 months shows complete healing of the fracture, and there is no evidence of avascular necrosis of femoral head or post-traumatic osteoarthritis.
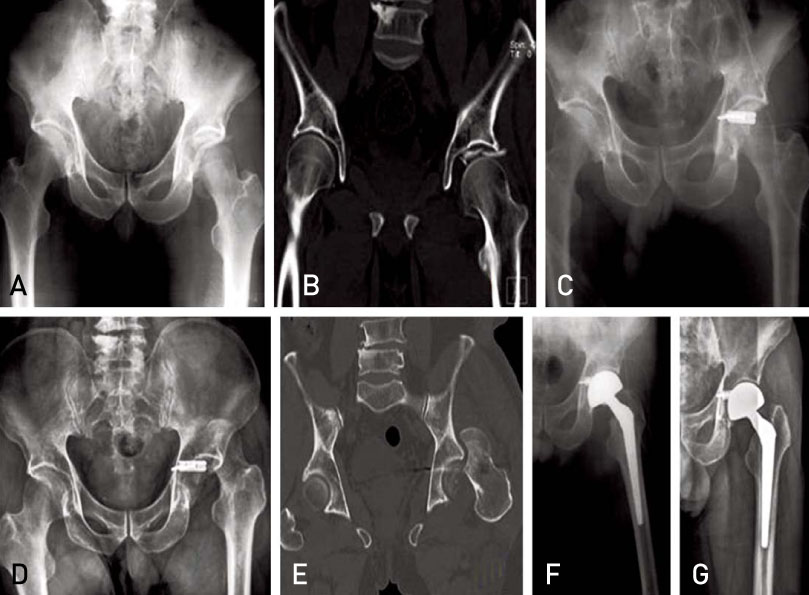
Fig. 2 (A, B) A 71-year-old male sustained Pipkin type IV fracture of hip. (C) Open reduction and internal fixation of acetabulum with spring plate and screws through the Kocher-Langenbeck approach was done. (D, E) The radiograph and CT at postoperative 2 months shows neglected posterior dislocation of hip. (F, G) Bipolar hemiarthroplasty of hip was done. The radiograph at postoperative 30 months shows well maintained prosthesis.
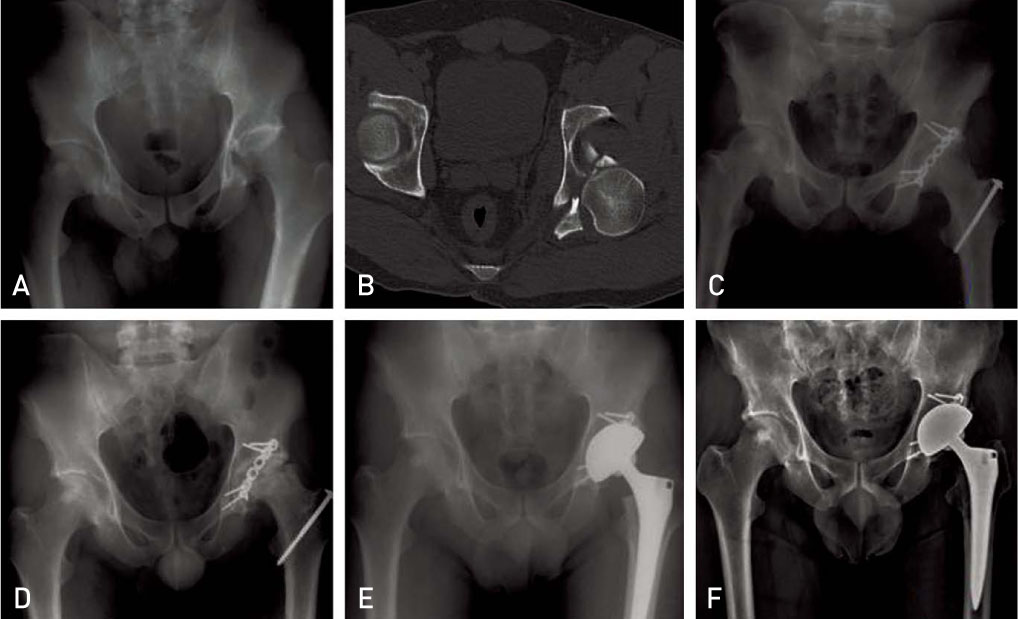
Fig. 3 (A, B) A 42-year-old male sustained Pipkin type IV fracture of hip. (C) Open reduction and internal fixation with reconstruction plate and screws through the Kocher-Langenbeck approach with trochanter flip osteotomy. (D) The radiograph at postoperative 21 months shows avascular necrosis of femoral head and osteoarthritis change on the joint. (E, F) Total hip arthroplasty was done. The radiograph at postoperative 96 months shows stable fixation of cup and stem.
Reference
-
1. Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip. 1987. 181–206.2. Butler JE. Pipkin Type-II fractures of the femoral head. J Bone Joint Surg Am. 1981. 63:1292–1296.
Article3. Epstein HC. Traumatic dislocations of the hip. Clin Orthop Relat Res. 1973. (92):116–142.
Article4. Thompson VP, Epstein HC. Traumatic dislocation of the hip; a survey of two hundred and four cases covering a period of twenty-one years. J Bone Joint Surg Am. 1951. 33-A:746–778. passim.5. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957. 39-A:1027–1042. passim.
Article6. Canale ST, Campbell WC. Campbell's operative orthopaedics. 1998. 9th ed. St. Louis: Mosby;2224–2234.7. Rockwood CA, Green DP, Heckman JD, Bucholz RW. Rockwood and Green's fractures in adults. 2001. 5th ed. Philadelphia: Lippincott Williams & Wilkins;1559–1560.8. Stimson LA. Five cases of dislocation of the hip. NY Med J. 1889. 50:118–121.9. Epstein HC. Posterior fracture-dislocations of the hip; long-term follow-up. J Bone Joint Surg Am. 1974. 56:1103–1127.10. Lyddon DW Jr, Hartman JT. Traumatic dislocation of the hip with ipsilateral femoral fractures. A case report. J Bone Joint Surg Am. 1971. 53:1012–1016.11. Gittins ME, Serif LW. Bilateral traumatic anterior/posterior dislocations of the hip joints: case report. J Trauma. 1991. 31:1689–1692.
Article12. Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res. 2000. (377):44–56.
Article13. Marchetti ME, Steinberg GG, Coumas JM. Intermediate-term experience of Pipkin fracture-dislocations of the hip. J Orthop Trauma. 1996. 10:455–461.
Article14. Watson-Jones R, Wilson JN. Watson-Jones Fractures and joint injuries. 1982. 6th ed. New York: Churchill Livingstone;885–934.15. Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res. 1985. (201):9–17.
Article16. Pape HC, Rice J, Wolfram K, Gansslen A, Pohlemann T, Krettek C. Hip dislocation in patients with multiple injuries. A follow up investigation. Clin Orthop Relat Res. 2000. (377):99–105.17. Kim JH, Lee SH, Moon YL, Kim DH, Song KS. Treatment of femoral head fracture with traumatic posterior dislocation of the hip. J Korean Hip Soc. 2007. 19:176–182.
Article18. Park MS, Rho CK. Clinical analysis of femoral head fracture. J Korean Orthop Assoc. 1992. 27:502–510.
Article19. Kloen P, Siebenrock KA, Raaymakers ELFB, Marti RK, Ganz R. Femoral head fractures revisited. Eur J Trauma. 2002. 28:221–233.
Article20. Hougaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg Am. 1988. 70:233–239.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Femoral Head Fracture without Hip Dislocation: A Case Report
- Hip Fracture-dislocation with Sciatic Nerve Palsy and Ipsilateral Femoral Shaft Open Fracture: A Case Report
- An Irreducible Hip Dislocation with Femoral Head Fracture
- Femoral Head Fracture with Hip Dislocation Treated by Autologous Osteochondral Transfer (Mosaicplasty) - A Case Report -
- A Traumatic Anterior Hip Dislocation Associated Ipsilateral Femoral Shaft Segmental Fracture : Case Report
