Preliminary Results for the Treatment of a Pain-Causing Osteoporotic Vertebral Compression Fracture with a Sky Bone Expander
- Affiliations
-
- 1Department of Orthopedics and Central Laboratory, Changzhou No 2. Hospital, Changzhou, China. jsczljb@yahoo.com.cn
- KMID: 1385400
- DOI: http://doi.org/10.3348/kjr.2008.9.5.420
Abstract
OBJECTIVE
Vertebral compression fractures (VCFs) are common complications of osteoporosis. The expansion of VCFs with a Sky Bone Expander is a new procedure which improves kyphotic deformities and decreases pain associated with VCFs. The purpose of this study was to investigate the preliminary results for the treatment of painful osteoporotic VCFs with a Sky Bone Expander. MATERIALS AND METHODS: Twenty-six patients with pain-causing VCFs were treated with a Sky Bone Expander. This operation involved the percutaneous insertion of the Sky Bone Expander into a fractured vertebral body transpedicularly. Following the expansion, the Sky Bone Expander was contracted and removed, resulting in a cavity to be filled with bone cement. All fractures were analyzed for improvement in sagittal alignment. Clinical complications, pain relief and ambulation status were evaluated 1 day, 1 week, 1 month, and 3 months after the operation. RESULTS: Twenty-four hours after the operation, all the patients treated experienced some degree of pain relief. In addition, no postoperative neurologic complications were noted. The average operative time was 42.4 +/- 15.5 min per vertebra. Moreover, an average cement volume of 3.5 mL (range, 2.5 +/- 5.0 mL) was injected per vertebra. The average anterior height was 18.4 +/- 5.1 mm preoperatively and 20.5 +/- 5.3 mm postoperatively (p < 0.01). Furthermore, the average midline height was 15.5 +/- 5.2 mm preoperatively and 18.9 +/- 4.0 mm postoperatively (p < 0.01). The Cobb angle improved from 18.5 +/- 8.2 degrees preoperatively to 9.2 +/- 4.0 degrees postoperatively (p < 0.01). The Visual Anabog Scale scores decreased from 7.7 +/- 1.8 points preoperatively to 3.1 +/- 2.0, 2.9 +/- 1.7, 2.6 +/- 1.5 and 2.9 +/- 11.3 after 1 day, 1 week, 1 month and 3 months after the operation, respectively. Cement extrusion was observed in four patients without any neurologic symptoms. CONCLUSION: As a result of this study, we can postulate that the expansion of compressed vetrebra with a Sky Bone Expander is a safe and minimally invasive procedure resulting in the restoration of vertebral body height and the relief of pain associated with VCFs.
MeSH Terms
-
Aged
Aged, 80 and over
Bone Cements
Female
Fractures, Compression/etiology/radiography/*surgery
Humans
Magnetic Resonance Imaging
Male
Middle Aged
Osteoporosis/*complications
Pain/etiology/*surgery
Postoperative Complications
Prospective Studies
Radiography, Thoracic
Spinal Fractures/etiology/radiography/*surgery
*Tissue Expansion Devices
Treatment Outcome
Figure
-
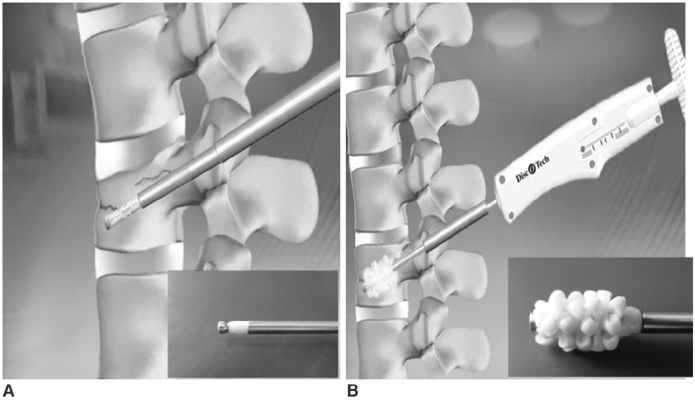
Fig. 1 Configurations of a Sky-bone expander. A. Before expansion B. After full expansion
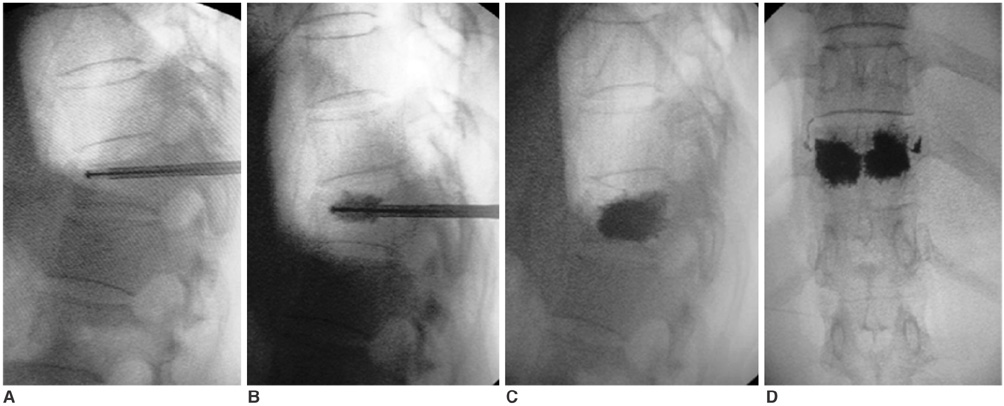
Fig. 2 Images of expansion of T11 osteoporotic vertebral compression fracture with Sky Bone Expander. A. Radiopaque polymer Expander was ideally situated under collapsed endplate in contracted configuration. B. Expander was unsheathed to elevate endplates. C, D. Lateral (C) and anteroposterior (D) radiographs showing vertebrae was filled with bone cement after Expander was resheathed and removed.
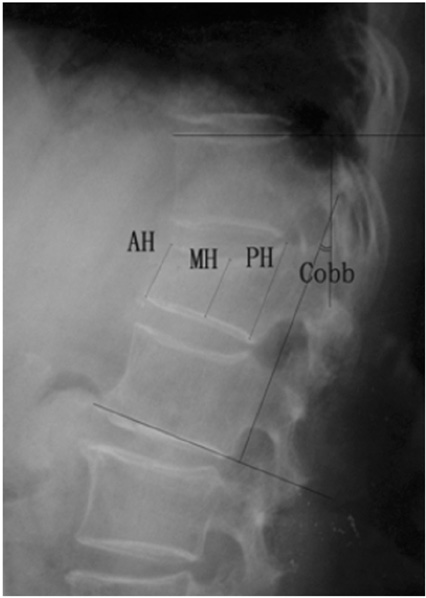
Fig. 3 Measurement of Cobb angle, anterior, middle, posterior vertebral height (AH, MH, PH).
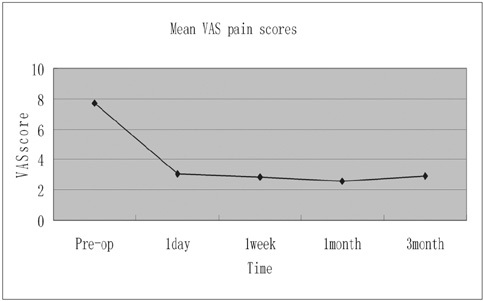
Fig. 4 Mean VAS (Visual Analog Scale) pain scores at all points.
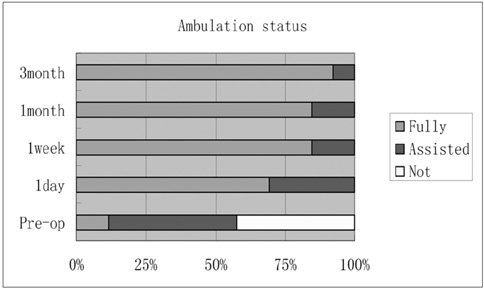
Fig. 5 Categorical ambulation status at all points.
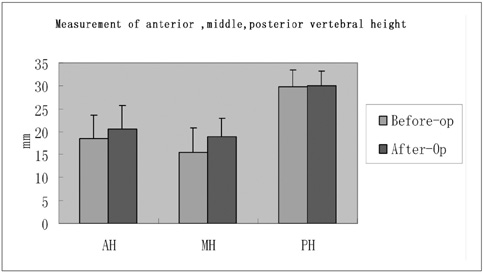
Fig. 6 Measurement of anterior, middle, posterior vertebral height at all points.

Fig. 7 Anteroposterior digital radiographs showing cement in paravertebral veins.
Reference
-
1. Jensen ME, Evans AJ, Mathis JM, Kallmes DF, Cloft HJ, Dion JE. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol. 1997. 18:1897–1904.2. Tong SC, Eskey CJ, Pomerantz SR, Hirsch JA. "Skyphoplasty": a single institution's initial experience. J Vasc Interv Radiol. 2006. 17:1025–1030.3. Zheng ZM, Kuang GM, Dong ZY, Cheung KM, Lu WW, Li FB. Preliminary clinical outcomes of percutaneous kyphoplasty with Sky-bone expander. Chin Med J (Engl). 2007. 120:761–766.4. Hu MM, Eskey CJ, Tong SC, Nogueira RG, Pomerantz SR, Rabinov JD, et al. Kyphoplasty for vertebral compression fracture via a uni-pedicular approach. Pain Physician. 2005. 8:363–367.5. Kuklo TR, Polly DW, Owens BD, Zeidman SM, Chang AS, Klemme WR. Measurement of thoracic and lumbar fracture kyphosis: evaluation of intraobserver, interobserver, and technique variability. Spine. 2001. 26:61–65.6. Heaney RP. The natural history of vertebral osteoporosis. Is low bone mass an epiphenomenon? Bone. 1992. 13:S23–SS2.7. Silverman SL. The clinical consequences of vertebral compression fracture. Bone. 1992. 13:S27–S31.8. Rao RD, Singrakhia MD. Painful osteoporotic vertebral fracture. J Bone Joint Surg Am. 2003. 85:2010–2022.9. Grohs JG, Matzner M, Trieb K, Krepler P. Minimal invasive stabilization of osteoporotic vertebral fractures: a prospective nonrandomized comparison of vertebroplasty and balloon kyphoplasty. J Spinal Disord Tech. 2005. 18:238–242.10. Laredo JD, Bellaiche L, Hamze B, Naouri JF, Bondeville JM, Tubiana JM. Current status of musculoskeletal interventional radiology. Radiol Clin North Am. 1994. 32:377–398.11. Cortet B, Cotten A, Boutry N, Flipo RM, Duquesnoy B, Chastanet P, et al. Percutaneous vertebroplasty in the treatment of osteoporotic vertebral compression fractures: an open prospective study. J Rheumatol. 1999. 26:2222–2228.12. Cyteval C, Sarrabere MP, Roux JO, Thomas E, Jorgensen C, Blotman F, et al. Acute osteoporotic vertebral collapse: open study on percutaneous injection of acrylic surgical cement in 20 patients. AJR Am J Roentgenol. 1999. 173:1685–1690.13. Deramond H, Depriester C, Galibert P, Le Gars D. Percutaneous vertebroplasty with polymethylmethacrylate. Technique, indications, and results. Radiol Clin North Am. 1998. 36:533–554.14. Voggenreiter G. Balloon kyphoplasty is effective in deformity correction of osteoporotic vertebral compression fractures. Spine. 2005. 30:2806–2812.15. Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine. 2001. 26:1511–1515.16. Ledlie JT, Renfro MB. Kyphoplasty treatment of vertebral fractures: 2-year outcomes show sustained benefits. Spine. 2006. 31:57–64.17. Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of "kyphoplasty" in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001. 26:1631–1638.18. Phillips FM, Todd Wetzel F, Lieberman I, Campbell-Hupp M. An in vivo comparison of the potential for extravertebral cement leak after vertebroplasty and kyphoplasty. Spine. 2002. 27:2173–2178.19. Phillips FM, Ho E, Campbell-Hupp M, McNally T, Todd Wetzel F, Gupta P. Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine. 2003. 28:2260–2267.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unilateral Biportal Endoscopy as a Treatment for Acute Radiculopathy after Osteoporotic Lumbar Compression Fracture: A Case Report
- The effect of percutaneous vertebroplasty with bone cement in the treatment of osteoporotic thoracolumbar compression fracture
- Complication of the Augmented Vertebral Body after Percutaneous Vertebroplasty in Patients with Osteoporotic Compression Fracture: Hammer Effect: Preliminary Report
- Risk Factors for Subsequent Fracture after Osteoporotic Vertebral Compression Fracture
- Correlation between Progression of Compression and Bone Densiometry Index in Osteoporotic Compression Fracture of Thoracolumbar Spine
