Frontoethmoidal Mucocele Presenting as Progressive Enophthalmos
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. yswoph@catholic.ac.kr
- 2Department of Otolaryngology-Head and Neck Surgery, Seoul St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea.
- KMID: 1376128
- DOI: http://doi.org/10.3341/kjo.2012.26.3.212
Abstract
- In this case report we describe a 27-year-old man who presented with progressive enophthalmos for 5 months without any other associated ocular symptoms such as pain, diplopia, or visual disturbance. Computed tomography showed that his progressive enophthalmos originated from a frontoethmoidal mucocele and this caused destruction of the lamina papyracea and shrinkage of the ethmoidal air cell. Finally the enlarged orbital space caused an inward deviation of the eyeball. Endoscopic marsupialization was successfully performed by an otolaryngologist and did not result in any ophthalmologic sequelae. Although frontoethmoidal sinus mucoceles mostly frequently originates from orbital mucoceles, enophthalmic manifestations are very rare. Enophthalmic conditions are not as responsive to surgical interventions as exophthalmic conditions.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Preoperative view of a 27-year-old man with right frontoethmoidal mucocele. Note the marked enophthalmos of right globe. (B) Preoerative computed tomography imaging: note the large right space occupying lesion from the frontal sinus extending toward ethmoid sinus. A destructive lesion of the lamina papyracea was found in the coronal view. (C) Preoperative magnetic resonance image imaging: the lesion showed T2 low signal intensity and T1 high signal intensity, which reflected the chronic state of frontoethmoidal mucocele.
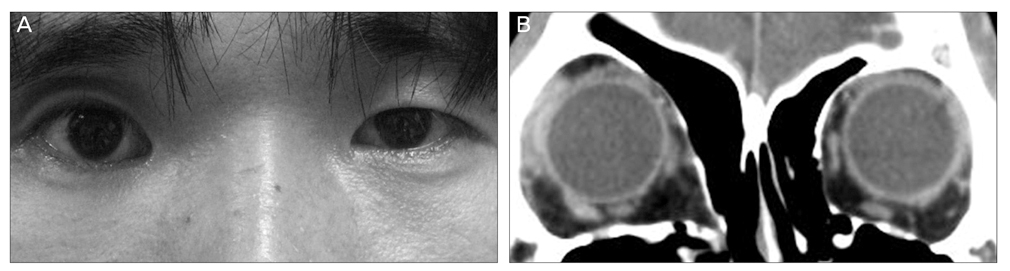
Fig. 2 (A) Postoperative view after 8 months showed that 3.0 mm enophthalmos of the right globe still remained. (B) Postoperative computed tomography imaging at same time showed resolution of the bony pseudocapsule and reformation of the orbit, which resulted in the deviation of right medial wall toward the ethmoidal sinus.
Reference
-
1. Hamedani M, Pournaras JA, Goldblum D. Diagnosis and management of enophthalmos. Surv Ophthalmol. 2007. 52:457–473.2. Annino DJ Jr, Goguen LA. Silent sinus syndrome. Curr Opin Otolaryngol Head Neck Surg. 2008. 16:22–25.3. McArdle B, Perry C. Ethmoid silent sinus syndrome caus ing inward displacement of the orbit: case report. J Laryngol Otol. 2010. 124:206–208.4. Braganza A, Khooshabeh R. Ethmoidal involvement in "imploding" (silent) sinus syndrome. Ophthal Plast Reconstr Surg. 2005. 21:305–307.5. Palmer-Hall AM, Anderson SF. Paraocular sinus mucoceles. J Am Optom Assoc. 1997. 68:725–733.6. Mineck CW, Chandra RK, Cohen N. Orbital mucopyocele after the use of alloplastic materials in the management of frontal sinus fractures. Otolaryngol Head Neck Surg. 2006. 135:974–976.7. Aitasalo KM, Peltola MJ. Bioactive glass hydroxyapatite in fronto-orbital defect reconstruction. Plast Reconstr Surg. 2007. 120:1963–1972.8. Girard B, Choudat L, Hamelin N, et al. Fronto-naso-eth moido-sphenoido-maxillo-orbital mucocele with ophthal-mologic presentation. J Fr Ophtalmol. 1999. 22:536–540.9. Wang TJ, Liao SL, Jou JR, Lin LL. Clinical manifestations and management of orbital mucoceles: the role of ophthalmologists. Jpn J Ophthalmol. 2005. 49:239–245.10. Chandra A, Lim M, Scott E, Morsman D. Frontoethmoidal mucocele associated with bilateral increased intraocular pressure and proptosis. Can J Ophthalmol. 2007. 42:143–144.11. Malhotra R, Wormald PJ, Selva D. Bilateral dynamic proptosis due to frontoethmoidal sinus mucocele. Ophthal Plast Reconstr Surg. 2003. 19:156–157.12. Shah A, Meyer DR, Parnes S. Management of frontoeth moidal mucoceles with orbital extension: is primary orbital reconstruction necessary? Ophthal Plast Reconstr Surg. 2007. 23:267–271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Separated Intraorbital Mucopyocele of Frontoethmoidal Sinus Origin
- A Case of Frontoethmoidal Mucopyocele Combined with Cerebrospinal Fluid Leak and Complicated Tension Pneumocephalus after Marsupialization
- Mucocele
- The Effect of Endonasal Dacryocystorhinostomy in the Paranasal Mucocele Invading Nasolacrimal Duct
- Medpor(R)-using Reconstruction of the Orbital Floor Defect Caused by the Maxillary Sinus Mucocele: A Case Report
