Spontaneous Resolution of Intravitreal Steroid-Induced Bilateral Cytomegalovirus Retinitis
- Affiliations
-
- 1Department of Ophthalmology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 2Gongdeok Seoul Eye Clinic, Seoul, Korea. imoon58@netsgo.com
- KMID: 1364872
- DOI: http://doi.org/10.3341/kjo.2012.26.2.151
Abstract
- A 73-year-old woman underwent vitrectomy and intravitreal triamcinolone acetonide (IVTA) of the right eye and cataract surgery with IVTA of the left eye, for bilateral diabetic macular edema. The patient presented with visual loss in both eyes three-months postoperatively. The fundoscopic examination revealed white-yellow, necrotic peripheral lesions in the superotemporal quadrant of both eyes. Although bilateral acute retinal necrosis was suspected, azotemia resulting from diabetic nephropathy limited the use of acyclovir. Antiviral treatment was not started. A sample of the aqueous humor for polymerase chain reaction (PCR) analysis was obtained. One week later, the PCR results indicated the presence of cytomegalovirus (CMV). Since the retinal lesions did not progress and did not threaten the macula, the patient was followed without treatment for CMV. The retinal lesions progressively regressed and completely resolved in both eyes by six months of follow-up. Patients with IVTA-induced CMV retinitis may not require systemic treatment with ganciclovir.
Keyword
MeSH Terms
-
Aged
Cataract Extraction
Cytomegalovirus Retinitis/*etiology
Diabetic Retinopathy/drug therapy/surgery
Female
Humans
Intravitreal Injections
Opportunistic Infections/*etiology
Remission, Spontaneous
Steroids/administration & dosage/*adverse effects
Triamcinolone Acetonide/administration & dosage/*adverse effects
Vitrectomy
Figure
-
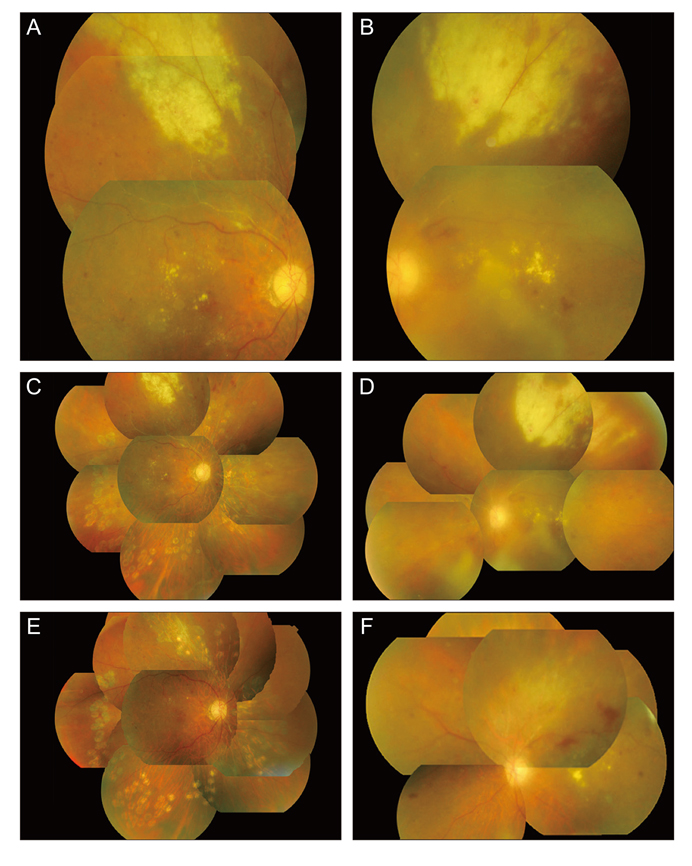
Fig. 1 (A,B) A 73-year-old woman, who underwent vitrectomy with intravitreal triamcinolone acetonide (IVTA) in the right eye and cataract surgery with IVTA in the left eye for bilateral diabetic macular edema, presented with visual loss in both eyes at three months post surgery. The fundus examination revealed white-yellow, necrotic peripheral lesions in the superotemporal quadrant of both eyes. The clinical impression was bilateral acute retinal necrosis. (C,D) Aqueous humor analyzed by polymerase chain reaction. The results were available seven days later and demonstrated the presence of cytomegalovirus. Meanwhile, despite no specific anti-cytomegalovirus treatment, the peripheral retinal lesion did not progress, and did not threaten the macula in both eyes. The patient was followed closely. (E,F) Six months later, the retinal lesions regressed completely with subsequent development of pigmentary changes of both eyes. A mild vitreous haze was still present in the left eye.
Reference
-
1. Wiegand TW, Young LH. Cytomegalovirus retinitis. Int Ophthalmol Clin. 2006. 46:91–110.2. Saidel MA, Berreen J, Margolis TP. Cytomegalovirus retinitis after intravitreous triamcinolone in an immunocompetent patient. Am J Ophthalmol. 2005. 140:1141–1143.3. Delyfer MN, Rougier MB, Hubschman JP, et al. Cytomegalovirus retinitis following intravitreal injection of triamcinolone: report of two cases. Acta Ophthalmol Scand. 2007. 85:681–683.4. Sekiryu T, Iida T, Kaneko H, Saito M. Cytomegalovirus retinitis after intravitreal triamcinolone acetonide in an immunocompetent patient. Jpn J Ophthalmol. 2008. 52:414–416.5. Park YS, Byeon SH. Cytomegalovirus retinitis after intravitreous triamcinolone injection in a patient with central retinal vein occlusion. Korean J Ophthalmol. 2008. 22:143–144.6. Ufret-Vincenty RL, Singh RP, Lowder CY, Kaiser PK. Cytomegalovirus retinitis after fluocinolone acetonide (Retisert) implant. Am J Ophthalmol. 2007. 143:334–335.7. Noffke AS, Mets MB. Spontaneous resolution of cytomegalovirus retinitis in an infant with congenital cytomegalovirus infection. Retina. 2001. 21:541–542.8. Whitcup SM, Cunningham ET Jr, Polis MA, Fortin E. Spontaneous and sustained resolution of CMV retinitis in patients receiving highly active antiretroviral therapy. Br J Ophthalmol. 1998. 82:845–846.9. Taylor-Wiedeman J, Sissons JG, Borysiewicz LK, Sinclair JH. Monocytes are a major site of persistence of human cytomegalovirus in peripheral blood mononuclear cells. J Gen Virol. 1991. 72(Pt 9):2059–2064.10. Bevan IS, Daw RA, Day PJ, et al. Polymerase chain reaction for detection of human cytomegalovirus infection in a blood donor population. Br J Haematol. 1991. 78:94–99.11. Stanier P, Kitchen AD, Taylor DL, Tyms AS. Detection of human cytomegalovirus in peripheral mononuclear cells and urine samples using PCR. Mol Cell Probes. 1992. 6:51–58.12. Docke WD, Prosch S, Fietze E, et al. Cytomegalovirus reactivation and tumour necrosis factor. Lancet. 1994. 343:268–269.13. Kondo K, Xu J, Mocarski ES. Human cytomegalovirus latent gene expression in granulocyte-macrophage progenitors in culture and in seropositive individuals. Proc Natl Acad Sci U S A. 1996. 93:11137–11142.14. Mendelson M, Monard S, Sissons P, Sinclair J. Detection of endogenous human cytomegalovirus in CD34+ bone marrow progenitors. J Gen Virol. 1996. 77(Pt 12):3099–3102.15. Fish KN, Soderberg-Naucler C, Mills LK, et al. Human cytomegalovirus persistently infects aortic endothelial cells. J Virol. 1998. 72:5661–5668.16. Fish KN, Stenglein SG, Ibanez C, Nelson JA. Cytomegalovirus persistence in macrophages and endothelial cells. Scand J Infect Dis Suppl. 1995. 99:34–40.17. Chen R, Xiong S, Yang Y, et al. The relationship between human cytomegalovirus infection and atherosclerosis development. Mol Cell Biochem. 2003. 249:91–96.18. Speir E, Modali R, Huang ES, et al. Potential role of human cytomegalovirus and p53 interaction in coronary restenosis. Science. 1994. 265:391–394.19. Rabinovitch T, Oh JO, Minasi P. In vivo reactivation of latent murine cytomegalovirus in the eye by immunosuppressive treatment. Invest Ophthalmol Vis Sci. 1990. 31:657–663.20. Vogel JU, Fleckenstein C, Wagner M, et al. The human eye (retina): a site of persistent HCMV infection? Graefes Arch Clin Exp Ophthalmol. 2005. 243:671–676.21. Halary F, Amara A, Lortat-Jacob H, et al. Human cytomegalovirus binding to DC-SIGN is required for dendritic cell infection and target cell trans-infection. Immunity. 2002. 17:653–664.22. Skiest DJ. Cytomegalovirus retinitis in the era of highly active antiretroviral therapy (HAART). Am J Med Sci. 1999. 317:318–335.23. Read RW, Zhang JA, Ishimoto SI, Rao NA. Evaluation of the role of human retinal vascular endothelial cells in the pathogenesis of CMV retinitis. Ocul Immunol Inflamm. 1999. 7:139–146.24. Beer PM, Bakri SJ, Singh RJ, et al. Intraocular concentration and pharmacokinetics of triamcinolone acetonide after a single intravitreal injection. Ophthalmology. 2003. 110:681–686.25. Mason JO 3rd, Somaiya MD, Singh RJ. Intravitreal concentration and clearance of triamcinolone acetonide in nonvitrectomized human eyes. Retina. 2004. 24:900–904.26. Lake KD, Fletcher CV, Love KR, et al. Ganciclovir pharmacokinetics during renal impairment. Antimicrob Agents Chemother. 1988. 32:1899–1900.27. McGavin JK, Goa KL. Ganciclovir: an update of its use in the prevention of cytomegalovirus infection and disease in transplant recipients. Drugs. 2001. 61:1153–1183.28. Whitcup SM, Fortin E, Nussenblatt RB, et al. Therapeutic effect of combination antiretroviral therapy on cytomegalovirus retinitis. JAMA. 1997. 277:1519–1520.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Intravitreal Ganciclovir Injection for Cytomegalovirus Retinitis
- A Case of Cytomegalovirus Retinitis Following Intravitreal Dexamethasone Implant in an Immunocompetent Patient with Uveitis
- Safety and Efficacy of Intravitreal Ganciclovir Injections More than 10 Times for Cytomegalovirus Retinitis
- Cytomegalovirus Retinitis after Intravitreal Bevacizumab Injection in an Immunocompetent Patient
- Ocular Ischemic Syndrome as the Initial Presenting Feature of Cytomegalovirus Retinitis
