Micropapillary Lung Cancer with Breast Metastasis Simulating Primary Breast Cancer due to Architectural Distortion on Images
- Affiliations
-
- 1Department of Diagnostic Radiology, Center for Breast Cancer, National Cancer Center, Goyang 410-769, Korea.
- 2Department of Pathology, Center for Breast Cancer, National Cancer Center, Goyang 410-769, Korea. JaeRo@tmhs.org
- 3Department of Pathology, The Methodist Hospital, Weill Medical College of Cornell University, Houston, TX, USA.
- 4Department of Surgery, Center for Breast Cancer, National Cancer Center, Goyang 410-769, Korea.
- KMID: 1245392
- DOI: http://doi.org/10.3348/kjr.2012.13.2.249
Abstract
- A 47-year-old Korean woman with right middle lobe lung adenocarcinoma, malignant pleural effusion, and multiple lymph node and bone metastases, after three months of lung cancer diagnosis, presented with a palpable right breast mass. Images of the right breast demonstrated architectural distortion that strongly suggested primary breast cancer. Breast biopsy revealed metastatic lung cancer with a negative result for estrogen receptor (ER), progesterone receptor (PR) and mammaglobin, and a positive result for thyroid transcription factor-1 (TTF-1). We present a case of breast metastasis from a case of lung cancer with an extensive micropapillary component, which was initially misinterpreted as a primary breast cancer due to unusual image findings with architectural distortion.
MeSH Terms
-
Adenocarcinoma/drug therapy/*secondary
Antineoplastic Combined Chemotherapy Protocols/therapeutic use
Biopsy, Needle
Bone Neoplasms/secondary
Breast Neoplasms/drug therapy/*secondary
Diagnosis, Differential
Female
Humans
Lung Neoplasms/*pathology
Lymphatic Metastasis
Mammography
Middle Aged
Neoplasm Staging
Tomography, X-Ray Computed
Ultrasonography, Mammary
Figure
-
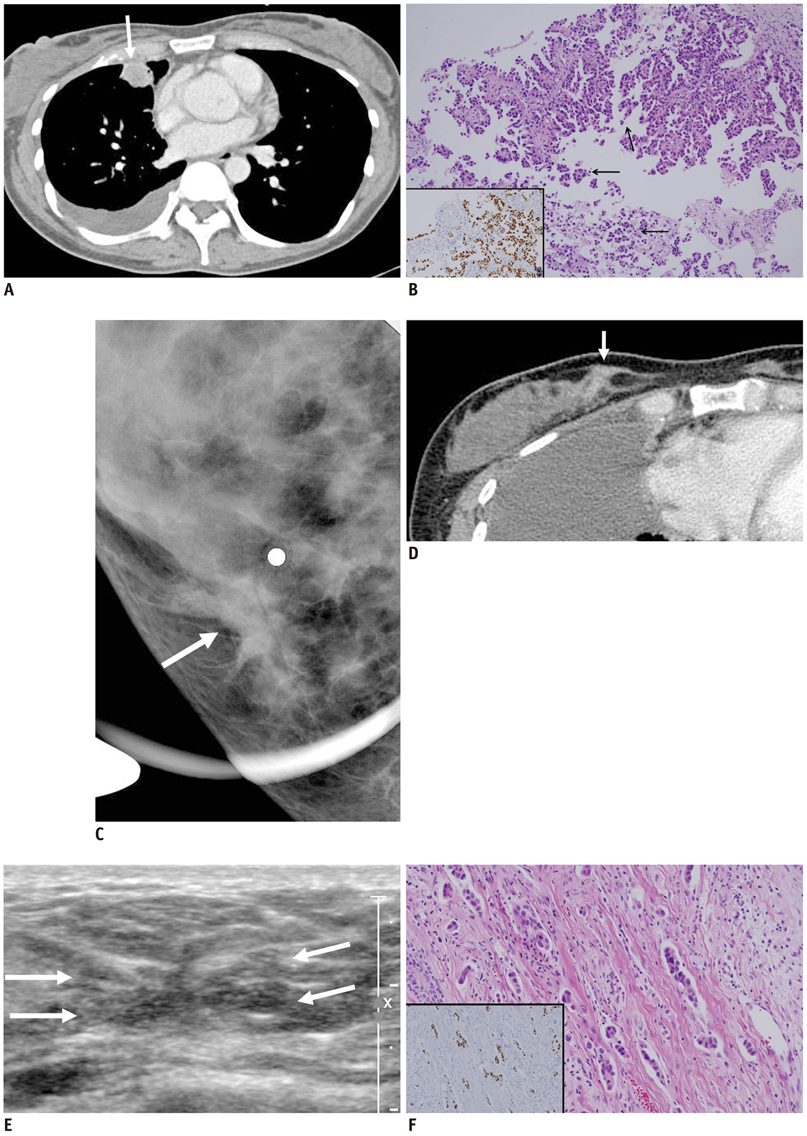
Fig. 1 Images and pathologic findings in 47-year-old woman with primary lung cancer. A. Outside chest CT shows round mass with internal necrosis in right middle lobe (arrow), with right pleural effusion. B. Primary lung cancer shows adenocarcinoma with papillary and micropapillary carcinoma (arrow; Hematoxylin and Eosin staining, × 100). TTF-1 stain reveals nuclear positivity (inset, TTF-1 immunostaining, × 200). C. Spot compression view of right breast shows focal architectural distortion (arrow) in right lower inner quadrant without evidence of microcalcifications or discrete mass. Metallic marker is attached to area of palpable site. D. Follow-up chest CT shows irregular enhancing lesion of right breast in lower inner quadrant (arrow). E. Breast US demonstrates 1 cm sized ill-defined irregular shaped isoechoic lesion (arrows) with focal infiltration at 4 o'clock position in right breast. F. Breast biopsy shows micropapillary carcinoma with small tumor cell nests in empty lacunar spaces and desmoplastic reaction in stroma (Hematoxylin and Eosin staining, × 100). TTF-1 stain reveals nuclear positivity, supporting metastasis from lung (TTF-1 immunostaining, × 100).
Reference
-
1. Lee SH, Park JM, Kook SH, Han BK, Moon WK. Metastatic tumors to the breast: mammographic and ultrasonographic findings. J Ultrasound Med. 2000. 19:257–262.2. Hajdu SI, Urban JA. Cancers metastatic to the breast. Cancer. 1972. 29:1691–1696.3. Vizcaíno I, Torregrosa A, Higueras V, Morote V, Cremades A, Torres V, et al. Metastasis to the breast from extramammary malignancies: a report of four cases and a review of literature. Eur Radiol. 2001. 11:1659–1665.4. Nassar H. Carcinomas with micropapillary morphology: clinical significance and current concepts. Adv Anat Pathol. 2004. 11:297–303.5. Amin MB, Tamboli P, Merchant SH, Ordóõez NG, Ro J, Ayala AG, et al. Micropapillary component in lung adenocarcinoma: a distinctive histologic feature with possible prognostic significance. Am J Surg Pathol. 2002. 26:358–364.6. Maeda R, Isowa N, Onuma H, Miura H, Harada T, Touge H, et al. Lung adenocarcinomas with micropapillary components. Gen Thorac Cardiovasc Surg. 2009. 57:534–539.7. Maounis N, Chorti M, Legaki S, Ellina E, Emmanouilidou A, Demonakou M, et al. Metastasis to the breast from an adenocarcinoma of the lung with extensive micropapillary component: a case report and review of the literature. Diagn Pathol. 2010. 5:82.8. Yang M, Nonaka D. A study of immunohistochemical differential expression in pulmonary and mammary carcinomas. Mod Pathol. 2010. 23:654–661.9. Gomez-Fernandez C, Mejias A, Walker G, Nadji M. Immunohistochemical expression of estrogen receptor in adenocarcinomas of the lung: the antibody factor. Appl Immunohistochem Mol Morphol. 2010. 18:137–141.10. Bhargava R, Beriwal S, Dabbs DJ. Mammaglobin vs GCDFP-15: an immunohistologic validation survey for sensitivity and specificity. Am J Clin Pathol. 2007. 127:103–113.11. Adrada B, Arribas E, Gilcrease M, Yang WT. Invasive micropapillary carcinoma of the breast: mammographic, sonographic, and MRI features. AJR Am J Roentgenol. 2009. 193:W58–W63.12. Paulus DD, Libshitz HI. Metastasis to the breast. Radiol Clin North Am. 1982. 20:561–568.13. Masmoudi A, Mathieu MC, Soria JC. Breast metastasis from lung adenocarcinoma: a case report. Anticancer Res. 2003. 23:1825–1826.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of stomach metastasis from breast cancer
- Metastatic Breast Cancer from Cervical Cancer
- Bladder Cancer Metastasis to the Breast in a Male Patient: Imaging Findings on Mammography and Ultrasonography
- Comment to “Patients with Concordant Triple-Negative Phenotype between Primary Breast Cancers and Corresponding Metastases Have Poor Prognosisâ€
- A Case of Small Cell Lung Cancer Metastastized to the Contralateral Breast
