Incidence and Management of Bleeding Complications Following Percutaneous Radiologic Gastrostomy
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 138-736, Korea. jhshin@amc.seoul.kr
- KMID: 1245381
- DOI: http://doi.org/10.3348/kjr.2012.13.2.174
Abstract
OBJECTIVE
Upper gastrointestinal (GI) bleeding is a serious complication that sometimes occurs after percutaneous radiologic gastrostomy (PRG). We evaluated the incidence of bleeding complications after a PRG and its management including transcatheter arterial embolization (TAE).
MATERIALS AND METHODS
We retrospectively reviewed 574 patients who underwent PRG in our institution between 2000 and 2010. Eight patients (1.4%) had symptoms or signs of upper GI bleeding after PRG.
RESULTS
The initial presentation was hematemesis (n = 3), melena (n = 2), hematochezia (n = 2) and bloody drainage through the gastrostomy tube (n = 1). The time interval between PRG placement and detection of bleeding ranged from immediately after to 3 days later (mean: 28 hours). The mean decrease in hemoglobin concentration was 3.69 g/dL (range, 0.9 to 6.8 g/dL). In three patients, bleeding was controlled by transfusion (n = 2) or compression of the gastrostomy site (n = 1). The remaining five patients underwent an angiography because bleeding could not be controlled by transfusion only. In one patient, the bleeding focus was not evident on angiography or endoscopy, and wedge resection including the tube insertion site was performed for hemostasis. The other four patients underwent prophylactic (n = 1) or therapeutic (n = 3) TAEs. In three patients, successful hemostasis was achieved by TAE, whereas the remaining one patient underwent exploration due to persistent bleeding despite TAE.
CONCLUSION
We observed an incidence of upper GI bleeding complicating the PRG of 1.4%. TAE following conservative management appears to be safe and effective for hemostasis.
MeSH Terms
Figure
-
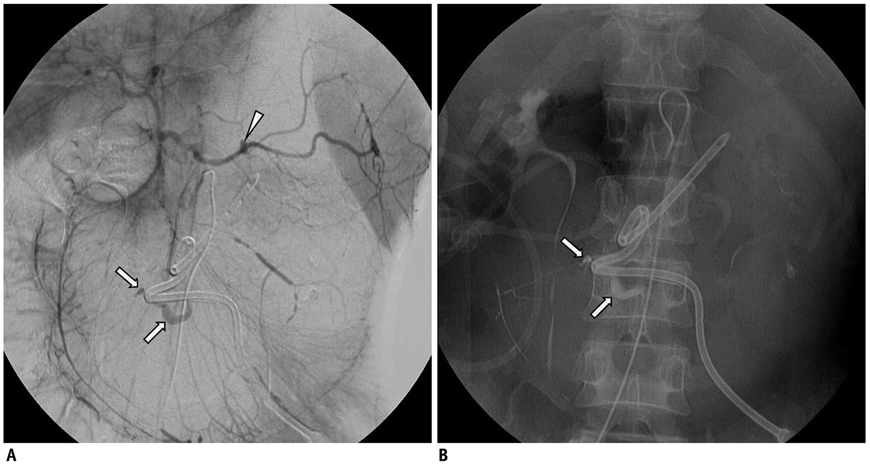
Fig. 1 Thirty two-year-old male patient with nasopharyngeal cancer (patient No. 2). A. Superior mesenteric angiogram shows extravasation from branch of right gastroepiploic artery (arrows) adjacent to tube. Pseudoaneurysm (arrowhead) in splenic artery caused by septic emboli is also observed. Due to retrograde flow with celiac stenosis, gastroepiploic artery and splenic artery are visualized on superior mesenteric angiogram. B. Successful N-butyl cyanoacrylate embolization (arrows) was done by superselection of bleeding focus at common hepatic artery level.
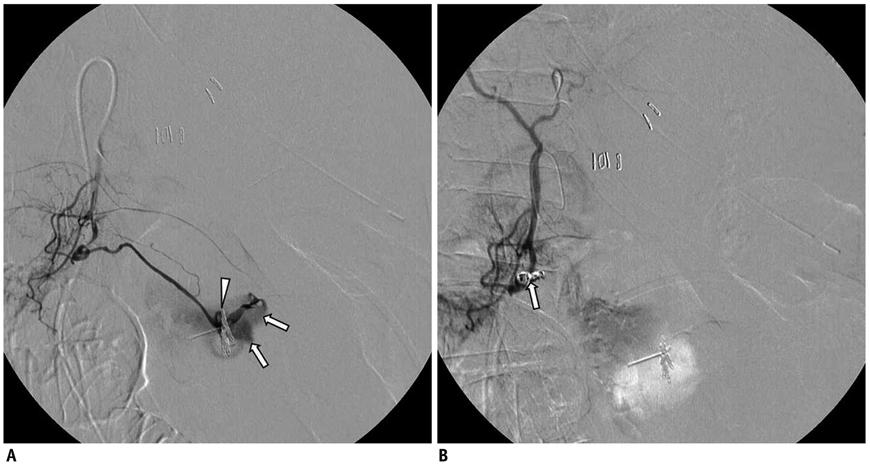
Fig. 2 Eighty seven-year-old female who previously underwent surgical repair of aortic dissection (patient No. 4). A. Right gastroepiploic angiogram shows extravasation (arrows) at greater curvature of stomach near hemoclips (arrowhead). B. Embolization with gelfoam slurry and microcoils (arrow) was performed at proximal part of bleeding focus due to marked tortuosity of right gastroepiploic artery. Splenic angiogram shows no collateral flow from left gastroepiploic artery (not shown). Although post-embolization angiogram shows no further bleeding, patient underwent laparotomy due to uncontrolled bleeding.
Reference
-
1. Laasch HU, Wilbraham L, Bullen K, Marriott A, Lawrance JA, Johnson RJ, et al. Gastrostomy insertion: comparing the options--PEG, RIG or PIG? Clin Radiol. 2003. 58:398–405.2. Dewald CL, Hiette PO, Sewall LE, Fredenberg PG, Palestrant AM. Percutaneous gastrostomy and gastrojejunostomy with gastropexy: experience in 701 procedures. Radiology. 1999. 211:651–656.3. Silas AM, Pearce LF, Lestina LS, Grove MR, Tosteson A, Manganiello WD, et al. Percutaneous radiologic gastrostomy versus percutaneous endoscopic gastrostomy: a comparison of indications, complications and outcomes in 370 patients. Eur J Radiol. 2005. 56:84–90.4. Möller P, Lindberg CG, Zilling T. Gastrostomy by various techniques: evaluation of indications, outcome, and complications. Scand J Gastroenterol. 1999. 34:1050–1054.5. Wollman B, D'Agostino HB, Walus-Wigle JR, Easter DW, Beale A. Radiologic, endoscopic, and surgical gastrostomy: an institutional evaluation and meta-analysis of the literature. Radiology. 1995. 197:699–704.6. Hicks ME, Surratt RS, Picus D, Marx MV, Lang EV. Fluoroscopically guided percutaneous gastrostomy and gastroenterostomy: analysis of 158 consecutive cases. AJR Am J Roentgenol. 1990. 154:725–728.7. Rose DB, Wolman SL, Ho CS. Gastric hemorrhage complicating percutaneous transgastric jejunostomy. Radiology. 1986. 161:835–836.8. Lewis MB, Lewis JH, Marshall H, Lossef SV. Massive hemorrhage complicating percutaneous endoscopic gastrostomy: treatment by means of transcatheter embolization of the right and left gastroepiploic arteries. J Vasc Interv Radiol. 1999. 10:319–323.9. Cappell MS, Godil A. A multicenter case-controlled study of percutaneous endoscopic gastrostomy in HIV-seropositive patients. Am J Gastroenterol. 1993. 88:2059–2066.10. Youn BJ, Hur J, Lee KH, Won JY. Transarterial embolization of massive gastric ulcer bleeding in gastrostomy patients caused by a balloon teplacement tube: a Case Report. J Korean Radiol Soc. 2007. 56:137–139.11. Nishiwaki S, Araki H, Takada J, Watanabe N, Asano T, Iwashita M, et al. Clinical investigation of upper gastrointestinal hemorrhage after percutaneous endoscopic gastrostomy. Dig Endosc. 2010. 22:180–185.12. Shin JH, Song HY, Kim TH, Kim KR, Choi KE, Kim JH. Percutaneous radiologic gastrostomy: a modified Chiba-needle puncture technique with single gastropexy. Abdom Imaging. 2010. 35:189–194.13. Kim JW, Song HY, Kim KR, Shin JH, Choi EK. The one-anchor technique of gastropexy for percutaneous radiologic gastrostomy: results of 248 consecutive procedures. J Vasc Interv Radiol. 2008. 19:1048–1053.14. Amann W, Mischinger HJ, Berger A, Rosanelli G, Schweiger W, Werkgartner G, et al. Percutaneous endoscopic gastrostomy (PEG). 8 years of clinical experience in 232 patients. Surg Endosc. 1997. 11:741–744.15. Larson DE, Burton DD, Schroeder KW, DiMagno EP. Percutaneous endoscopic gastrostomy. Indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology. 1987. 93:48–52.16. Rabeneck L, Wray NP, Petersen NJ. Long-term outcomes of patients receiving percutaneous endoscopic gastrostomy tubes. J Gen Intern Med. 1996. 11:287–293.17. Mamel JJ. Percutaneous endoscopic gastrostomy. Am J Gastroenterol. 1989. 84:703–710.18. Rimon E. The safety and feasibility of percutaneous endoscopic gastrostomy placement by a single physician. Endoscopy. 2001. 33:241–244.19. Shellito PC, Malt RA. Tube gastrostomy. Techniques and complications. Ann Surg. 1985. 201:180–185.20. Wasiljew BK, Ujiki GT, Beal JM. Feeding gastrostomy: complications and mortality. Am J Surg. 1982. 143:194–195.21. Cappell MS, Iacovone FM Jr. The safety and efficacy of percutaneous endoscopic gastrostomy after recent myocardial infarction: a study of 28 patients and 40 controls at four university teaching hospitals. Am J Gastroenterol. 1996. 91:1599–1603.22. Cheung FK, Lau JY. Management of massive peptic ulcer bleeding. Gastroenterol Clin North Am. 2009. 38:231–243.23. Elmunzer BJ, Young SD, Inadomi JM, Schoenfeld P, Laine L. Systematic review of the predictors of recurrent hemorrhage after endoscopic hemostatic therapy for bleeding peptic ulcers. Am J Gastroenterol. 2008. 103:2625–2632. quiz 2633.24. Lee HJ, Shin JH, Yoon HK, Ko GY, Gwon DI, Song HY, et al. Transcatheter arterial embolization in gastric cancer patients with acute bleeding. Eur Radiol. 2009. 19:960–965.25. Burke SJ, Golzarian J, Weldon D, Sun S. Nonvariceal upper gastrointestinal bleeding. Eur Radiol. 2007. 17:1714–1726.26. Aina R, Oliva VL, Therasse E, Perreault P, Bui BT, Dufresne MP, et al. Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol. 2001. 12:195–200.27. Morris DC, Nichols DM, Connell DG, Burhenne HJ. Embolization of the left gastric artery in the absence of angiographic extravasation. Cardiovasc Intervent Radiol. 1986. 9:195–198.28. Sos TA, Lee JG, Wixson D, Sniderman KW. Intermittent bleeding from minute to minute in acute massive gastrointestinal hemorrhage: arteriographic demonstration. AJR Am J Roentgenol. 1978. 131:1015–1017.29. McClave SA, Chang WK. Complications of enteral access. Gastrointest Endosc. 2003. 58:739–751.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Updates on Percutaneous Radiologic Gastrostomy/Gastrojejunostomy and Jejunostomy
- Percutaneous Radiologic Gastrostomy in a Locked-in Syndrome Patient : A case report
- Percutaneous Endoscopic Gastrostomy Versus Percutaneous Radiologic Gastrostomy: A Comparison of Complications in Brain Injured Patients
- A Case of Severe Gastric Ulcer Bleeding after Exchange for Replacement Balloon Gastrostomy Tube in Percutaneous Endoscopic Gastrostomy
- Percutaneous Endoscopic Gastrostomy: Procedure, Complications and Management
