Morton Neuroma: Evaluated with Ultrasonography and MR Imaging
- Affiliations
-
- 1Department of Diagnostic Radiology and the Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea. jss@yumc.yonsei.ac.kr
- 2Department of Diagnostic Radiology, Hanyang University College of Medicine, Kuri City, Kyunggi-do, Korea.
- 3Department of Diagnostic Radiology, Seoul Medical Center, Seoul, Korea.
- 4Department of Orthopedics, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1126838
- DOI: http://doi.org/10.3348/kjr.2007.8.2.148
Abstract
OBJECTIVE
The purpose of this study was to compare the diagnostic accuracy of both ultrasonography (US) and magnetic resonance imaging (MRI) for the assessment of Morton neuroma. MATERIALS AND METHODS: Our study group was comprised of 20 neuromas from 17 patients, and the neuromas were confirmed on surgery following evaluation with US, MRI, or both US and MRI. The diagnostic criterion for Morton neuroma, as examined by US, was the presence of a round or ovoid, well-defined, hypoechoic mass. The diagnostic criterion, based on MR imaging, was a well defined mass with intermediate to low signal intensity on both the T1- and T2-weighted images. The retrospective comparison between the sonographic and MR images was done by two experienced radiologists working in consensus with the surgical and pathologic correlations. RESULTS: The detection rate of Morton neuroma was 79% for 14 neuromas from 11 patients who had undergone US followed by an operation. The detection rate was 76% for 17 neuromas from 15 patients who had undergone MRI and a subsequent operation. The mean size of the examined neuromas was 4.9 mm on the US images and it was 5.1 mm on the MRI studies. Ten neuromas (71%) were 5 mm or less as measured by US, and three neuromas were not detected, whereas on the MRI analysis, 10 neuromas (59%) were 5 mm or less and four neuromas were not visualized. Among the patients examined during postoperative follow-up, symptoms were completely relieved in 85% and the symptoms were partially relieved in 15%. CONCLUSION: US and MR imaging are comparable modalities with high detection rate for the evaluation of Morton neuroma.
Keyword
MeSH Terms
Figure
-
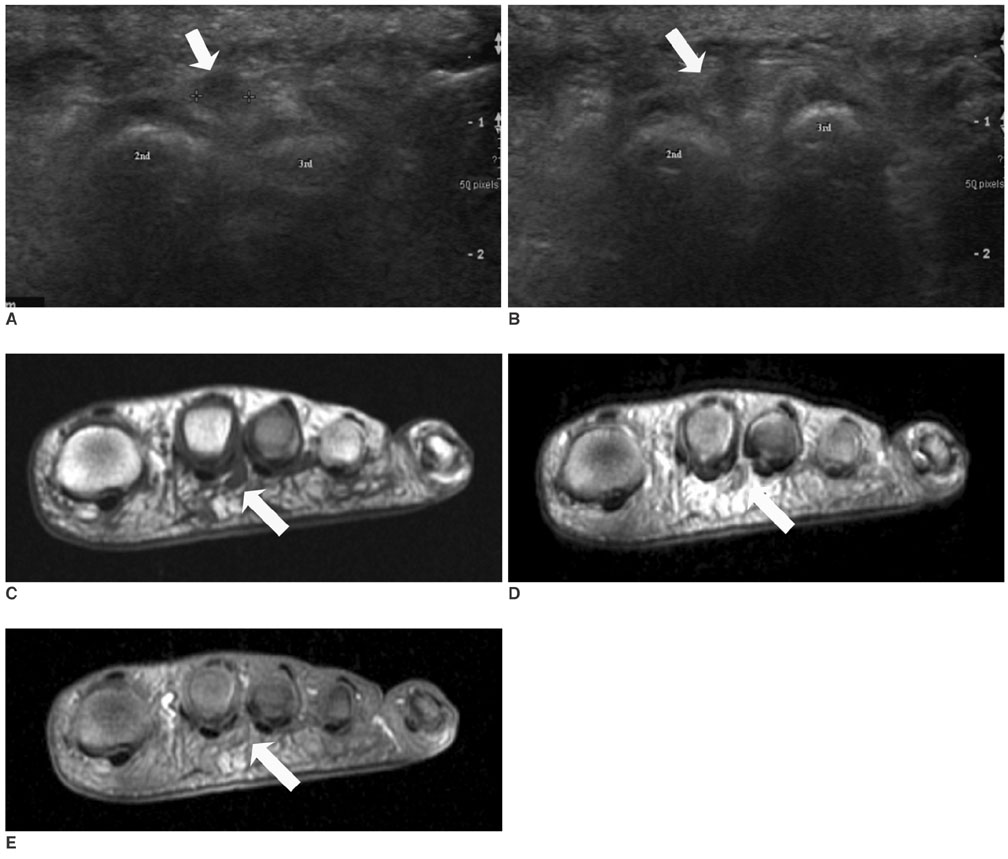
Fig. 1 Morton neuroma in the second intermetatarsal space in a 56-year-old woman (patient number 1 in table 1). She experienced pain in the second intermetatarsal space on the left foot. A, B. Sonogram of the second intermetatarsal space in the coronal plane shows a 4 mm-sized, ovoid, hypoechoic nodule (arrow) between the 2nd and 3rd metatarsal heads. C. The T1-weighted spin-echo MR image (TR/TE = 550/9) shows a well-demarcated 5-mm-sized, hypo-intense soft-tissue nodule (arrow) in the second intermetatarsal space. D. The FSE T2-weighted MR image (TR/TE = 4000/96) shows areas of slightly increased signal intensity within the neuroma (arrow). E. The T1-weighted fat-suppressed contrast-enhanced spin-echo MR image (TR/TE = 617/12) shows mild enhancement in the nodule (arrow).
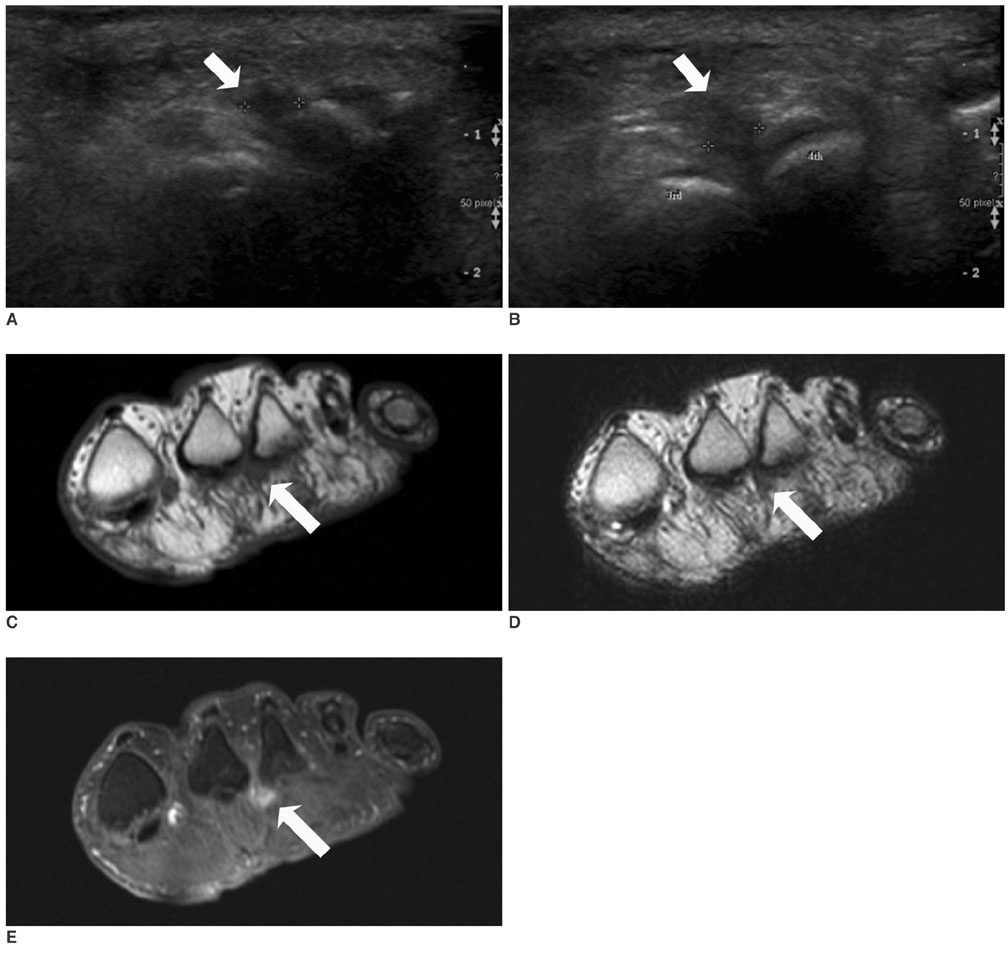
Fig. 2 Morton neuroma in the second and third intermetatarsal spaces in a 55-year-old woman (patient number 16 in table 1). The patient had suffered from metatarsalgia in the third intermetatarsal space on the left foot. A, B. The sonogram of the third intermetatarsal space in the sagittal (A) and coronal (B) planes shows a 4 mm-sized, ovoid, hypoechoic nodule (arrows) in the 3rd intermetatarsal space. No abnormal lesion is seen in the second space. C. Instead, the T1-weighted spin-echo MR image (TR/TE = 550/9) shows a well-demarcated, 5 mm-sized, hypointense soft-tissue nodule (arrow) in the second intermetatarsal space. D. The FSE T2-weighted MR image (TR/TE = 4000/96) shows hyperintensity within the neuroma (arrow). E. The T1-weighted fat-suppressed contrast-enhanced spin-echo MR image (TR/TE = 617/12) shows homogeneous enhancement of the nodule (arrow). No abnormal finding is seen in the third intermetatarsal space. At operation, both the 2nd and 3rd plantar nerves were thickened and neurolysis was performed on these two nerves. The patient's pain was relieved after the operation.
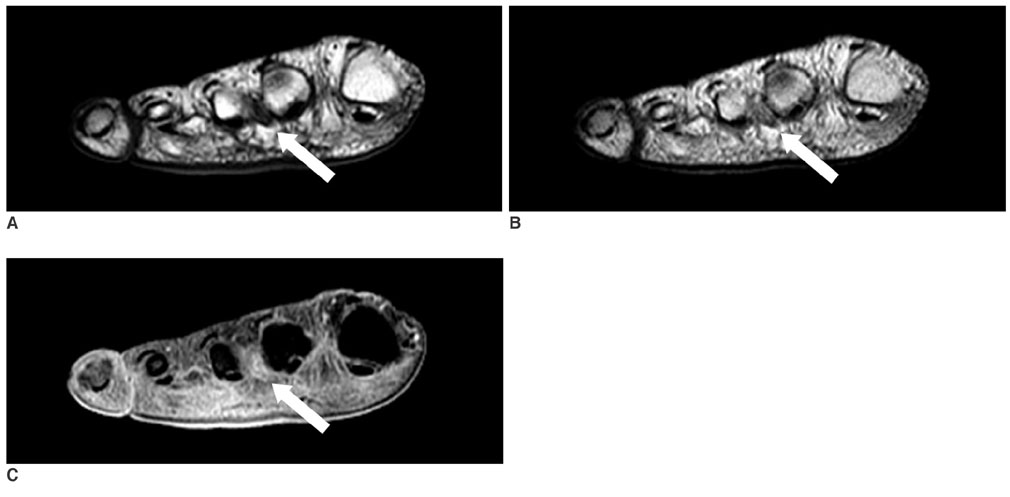
Fig. 3 Morton neuroma in the third intermetatarsal space in a 59-year-old woman (patient number 3 in table 1). Only MRI was performed. A. The T1-weighted spin-echo MR image (TR/TE = 483/11) shows a well-demarcated, 5 mm-sized, hypointense soft-tissue nodule (arrow) in the second intermetatarsal space. B. The FSE T2-weighted MR image (TR/TE = 5400/96) shows areas of slightly increased signal intensity within the neuroma (arrow). C. The T1-weighted fat-suppressed contrast-enhanced spin-echo MR image (TR/TE = 683/11) shows mild enhancement of the nodule (arrow). An operation was performed on only the 3rd intermetatarsal space because of metatarsalgia in this area, and a thick 1-cm-sized neuroma was excised. The second intermetatarsal space was not confirmed as containing neuroma during the operation.
Reference
-
1. Zanetti M, Ledermann T, Zollinger H, Hodler J. Efficacy of MR imaging in patients suspected of having Morton's neuroma. AJR Am J Roentgenol. 1997. 168:529–532.2. Wu KK. Morton neuroma and metatarsalgia. Curr Opin Rheumatol. 2000. 12:131–142.3. Zanetti M, Strehle JK, Zollinger H, Hodler J. Morton neuroma and fluid in the intermetatarsal bursae on MR images of 70 asymptomatic volunteers. Radiology. 1997. 203:516–520.4. Bencardino J, Rosenberg ZS, Beltran J, Liu X, Marty-Delfaut E. Morton's neuroma: is it always symptomatic? AJR Am J Roentgenol. 2000. 175:649–653.5. Redd RA, Peters VJ, Emery SF, Branch HM, Rifkin MD. Morton neuroma: sonographic evaluation. Radiology. 1989. 171:415–417.6. Pollak RA, Bellacosa RA, Dornbluth NC, Strash WW, Devall JM. . J Foot Surg. 1992. 31:534–537.7. Biasca N, Zanetti M, Zollinger H. Outcomes after partial neurectomy of Morton's neuroma related to preoperative case histories, clinical findings, and findings on magnetic resonance imaging scans. Foot Ankle Int. 1999. 20:568–575.8. Zanetti M, Strehle JK, Kundert HP, Zollinger H, Hodler J. Morton neuroma: effect of MR imaging findings on diagnostic thinking and therapeutic decisions. Radiology. 1999. 213:583–588.9. Shapiro PP, Shapiro SL. Sonographic evaluation of interdigital neuromas. Foot Ankle Int. 1995. 16:604–606.10. Kaminsky S, Griffin L, Milsap J, Page D. Is ultrasonography a reliable way to confirm the diagnosis of Morton's neuroma? Orthopedics. 1997. 20:37–39.11. Sharp RJ, Wade CM, Hennessy MS, Saxby TS. The role of MRI and ultrasound imaging in Morton's neuroma and the effect of size of lesion on symptoms. J Bone Joint Surg Br. 2003. 85:999–1005.12. Terk MR, Kwong PK, Suthar M, Horvath BC, Colletti PM. Morton neuroma: evaluation with MR imaging performed with contrast enhancement and fat suppression. Radiology. 1993. 189:239–241.13. Williams JW, Meaney J, Whitehouse GH, Klenerman L, Hussein Z. MRI in the investigation of Morton's neuroma: which sequences? Clin Radiol. 1997. 52:46–49.14. Johnson JE, Johnson KA, Unni KK. Persistent pain after excision of an interdigital neuroma. Results of reoperation. J Bone Joint Surg Am. 1988. 70:651–657.15. Weishaupt D, Treiber K, Kundert HP, Zollinger H, Vienne P, Hodler J, et al. Morton neuroma: MR imaging in prone, supine, and upright weight-bearing body positions. Radiology. 2003. 226:849–856.16. Erickson SJ, Canale PB, Carrera GF, Johnson JE, Shereff MJ, Gould JS, et al. Interdigital (Morton) neuroma: high-resolution MR imaging with a solenoid coil. Radiology. 1991. 181:833–836.17. Quinn TJ, Jacobson JA, Craig JG, van Holsbeeck MT. Sonography of Morton's neuromas. AJR Am J Roentgenol. 2000. 174:1723–1728.18. Wu KK. Morton's interdigital neuroma: a clinical review of its etiology, treatment, and results. J Foot Ankle Surg. 1996. 35:112–119. discussion 187-188.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasonography of Morton's Neuroma Accompanied with Interdigital Bursitis
- Clinical Result of Conservative Treatment and Operative Treatment for Interdigital Neuroma
- The Comparison of Ultrasonographic Size of Morton's Neuroma measured to Actual Size
- Morton's Neuroma
- A Clinical Result of Treatment of Interdigital Neuroma with Decompression (4 Cases Report)
