Yonsei Med J.
2007 Oct;48(5):883-885. 10.3349/ymj.2007.48.5.883.
Acute Myocardial Infarction Due to an Unruptured Sinus of Valsalva Aneurysm in a Patient with Behcet's Syndrome
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Yonsei Cardiovascular Center, Yonsei University College of Medicine, Seoul, Korea. kjy@yuhs.ac
- KMID: 1122631
- DOI: http://doi.org/10.3349/ymj.2007.48.5.883
Abstract
- This report describes the case of a 45-year-old Korean female who had suffered from Behcet's syndrome for two years with a huge, unruptured aneurysm originating from the left coronary sinus. The aneurysm had caused myocardial and aortic insufficiency by compressing the proximal left anterior descending coronary artery. The orifice of the aneurysm was at the left coronary sinus, about 5mm from the left main coronary ostium, and it was filled with organized thrombi. Surgical repair was performed by closing the entrance of the aneurysm with a Dacron patch and by implementing aortic valve repair and coronary artery bypass grafting. The patient's coronary flow was restored postoperatively, and all anginal symptoms disappeared.
Keyword
MeSH Terms
Figure
-
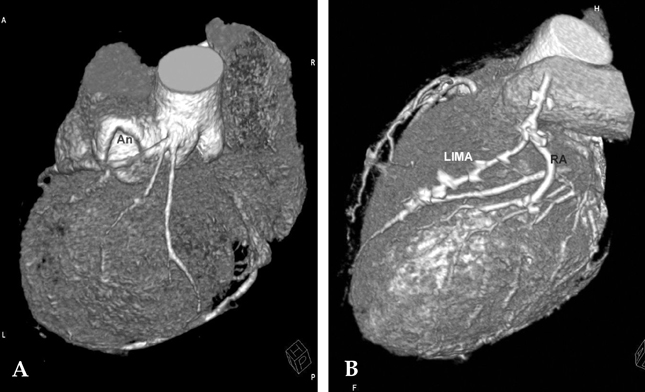
Fig. 1 (A) Preoperative MD-CT showed a dilated left SVA with a huge aneurysm (An) compressing the left coronary artery. (B) Postoperative MD-CT showed patent left internal mammary (LIMA) and radial artery (RA) bypass grafts, with a regressed aneurysm.
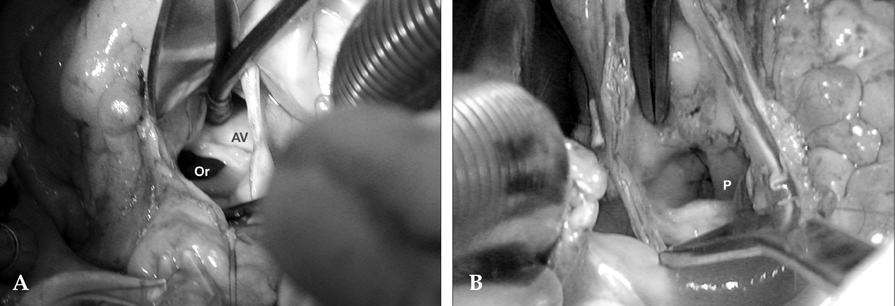
Fig. 2 (A) The orifice of the aneurysm (Or) was observed at the left SVA, originating about 5mm from the left main coronary ostium, and was filled with organized mural thrombi. (B) The orifice of the aneurysm was closed with a patch (P), and then aortic valvuloplasty was performed.
Reference
-
1. Kusuyama T, Nakamura Y, Yamagishi H, Shimada K, Watanabe H, Muro T, et al. Unruptured aneurysm of the sinus of valsalva with Beçhet's disease. Circ J. 2002. 66:107–108.
Article2. Okada K, Eishi K, Kitoh Y, Kosakai Y, Isobe F, Nakano K, et al. Huge aneurysm of the sinus of Valsalva following infective endocarditis in Beçhet's disease. J Heart Valve Dis. 1997. 6:179–180.3. Wakabayashi Y, Tawarahara K, Kurata C. Aneurysms of all sinuses of Valsalva and aortic valve prolapse secondary to Beçhet's disease. Eur Heart J. 1996. 17:1766.
Article4. Takach TJ, Reul GJ, Duncan JM, Cooley DA, Livesay JJ, Ott DA, et al. Sinus of Valsalva aneurysm or fistula: management and outcome. Ann Thorac Surg. 1999. 68:1573–1577.
Article5. Kutay V, Ekim H, Yakut C. Surgical repair of postoperative left sinus of Valsalva aneurysm dissecting into the interventricular septum. Ann Thorac Surg. 2005. 79:341–343.
Article6. Chung HJ, Goo BC, Lee JH, Bang D, Lee KH, Lee ES, et al. Beçhet's disease combined with various types of fistula. Yonsei Med J. 2005. 46:625–628.
Article7. Harkness JR, Fitton TP, Barreiro CJ, Alejo D, Gott VL, Baumgartner WA, et al. A 32-year experience with surgical repair of sinus of Valsalva aneurysms. J Card Surg. 2005. 20:198–204.
Article8. Vural KM, Sener E, Tasdemir O, Bayazit K. Approach to sinus of Valsalva aneurysms: a review of 53 cases. Eur J Cardiothorac Surg. 2001. 20:71–76.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Rare Case of Unruptured Sinus of Valsalva Aneurysm Obstructing the Right Ventricular Outflow Tract
- Huge Aneurysm of the Sinus of Valsalva Compressing the Left Atrium
- Unruptured Aneurysm of the Left Sinus of Valsalva Presenting as Acute Coronary Syndrome: A Case Report
- A Case of Ruptured Aneurysm of the Sinus of Valsalva into the Left Ventricle with Complete AV Block in Behcet's Syndrome
- Sudden Cardiac Death from Acute Myocardial Infarction Caused by Unruptured Ascending Aortic Aneurysm Involving the Sinus of Valsalva: An Autopsy Case
