The Diagnostic Accuracy, Image Quality and Radiation Dose of 64-Slice Dual-Source CT in Daily Practice: a Single Institution's Experience
- Affiliations
-
- 1Department of Radiology and the Institute of Radiation Medicine, Seoul National University College of Medicine, Clinical Research Institute, Seoul National University Hospital, Seoul 110-744, Korea. iameuna1@gmail.com
- 2Department of Internal Medicine and the Cardiovascular Center, Seoul National University Hospital, Seoul 110-744, Korea.
- KMID: 1122328
- DOI: http://doi.org/10.3348/kjr.2011.12.3.308
Abstract
OBJECTIVE
We wanted to evaluate the image quality, diagnostic accuracy and radiation exposure of 64-slice dual-source CT (DSCT) coronary angiography according to the heart rate in symptomatic patients during daily clinical practice.
MATERIALS AND METHODS
We performed a retrospective search for the DSCT coronary angiography reports of 729 consecutive symptomatic patients. For the 131 patients who underwent invasive coronary angiography, the image quality, the diagnostic performance (sensitivity, specificity, positive predictive value [PPV] and negative predictive value [NPV] for detecting significant stenosis > or = 50% diameter) and the radiation exposure were evaluated. These values were compared between the groups with differing heart rates (HR): mean HR < 65 or > or = 65 and HR variability (HRV) < 15 or > or = 15.
RESULTS
Among the 729 patients, the CT reports showed no stenosis or insignificant coronary artery stenosis in 72%, significant stenosis in 26% and non-diagnostic in 2%. For the 131 patients who underwent invasive coronary angiography, 95% of the patients and 97% of the segments were evaluable, and the overall per-patient/per-segment sensitivity, the perpatient/per-segment specificity, the per-patient/per-segment PPV and the per-patient/per-segment NPV were 100%/90%, 71%/98%, 95%/88% and 100%/97%, respectively. The image quality was better in the HR < 65 group than in the HR > or = 65 group (p = 0.001), but there was no difference in diagnostic performance between the two groups. The mean effective radiation doses were lower in the HR < 65 or HRV < 15 group (p < 0.0001): 5.5 versus 6.7 mSv for the mean HR groups and 5.3 versus 9.3 mSv for the HRV groups.
CONCLUSION
Dual-source CT coronary angiography is a highly accurate modality in the clinical setting. Better image quality and a significant radiation reduction are being rendered in the lower HR group.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Artifacts
Contrast Media/diagnostic use
Coronary Angiography/*methods
Coronary Stenosis/*radiography
Female
Humans
Imaging, Three-Dimensional
Male
Middle Aged
Predictive Value of Tests
Quality Assurance, Health Care
Radiation Dosage
Radiographic Image Interpretation, Computer-Assisted/methods
Retrospective Studies
Sensitivity and Specificity
Tomography, X-Ray Computed/*methods
Figure
-

Fig. 1 Flow chart for routine work-up for 729 patients who underwent 64-slice dual-source CT coronary angiography. Treadmill test or myocardial single photon emission CT (SPECT) was performed within one month before or after dual-source CT coronary angiography. Invasive coronary angiography was performed within three months after dual-source CT coronary angiography.
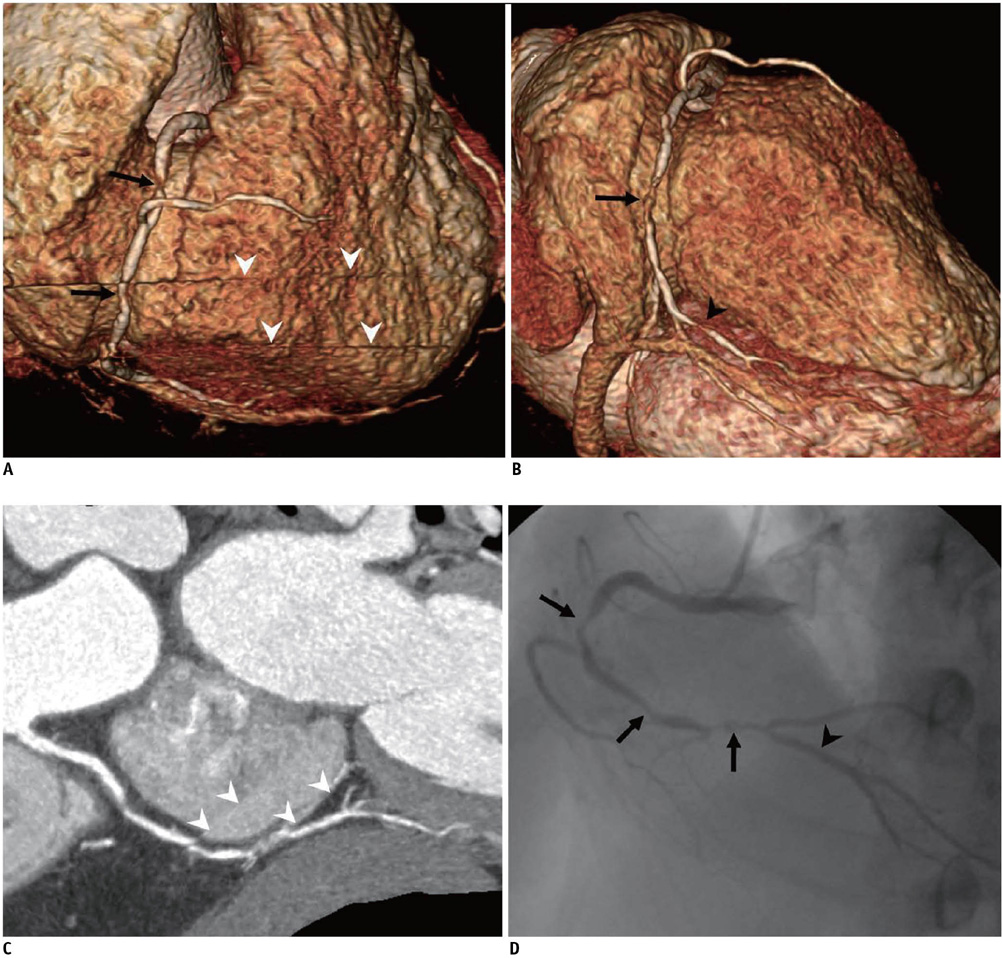
Fig. 2 Coronary angiography in 65-year-old male with mean heart rate of 48 beats per minute (bpm) and his heart rate variability was 15 bpm. Volume CT dose index (CTDIvol) and effective dose were 21.1 mGy and 5.4 mSv, respectively. CT volume-rendered reconstruction (A, B) and conventional angiogram (D) show significant stenosis of right coronary artery (arrows). Mild degree of severe stair-step artifacts (white arrowheads) was observed on volume-rendered reconstruction (A) and curved multiplanar reconstruction (C). Of note, severe stenosis of posterior descending coronary artery (black arrowhead) was also seen on volume-rendered reconstruction (B). Conventional angiogram (D) taken on same day does not show stenosis of posterior descending artery (arrowhead). This is false positive case.
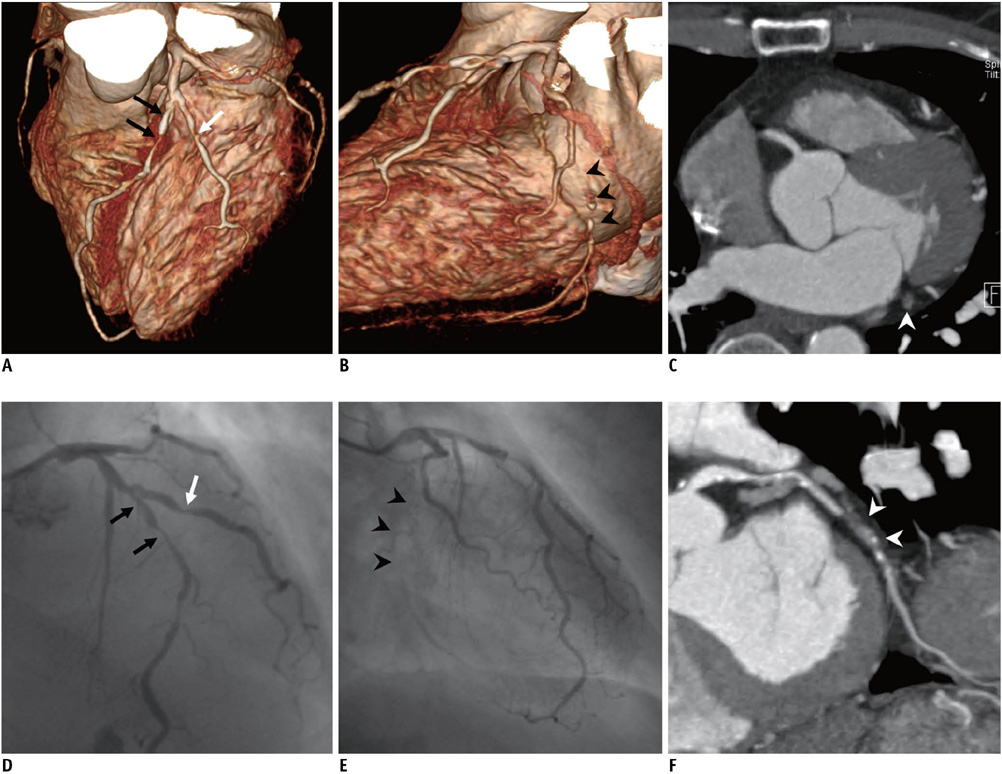
Fig. 3 Coronary angiography in 54-year-old male with mean heart rate of 63 beats per minute (bpm) and his heart rate variability was 5 bpm. Volume CT dose index (CTDIvol) and effective dose were 18.0 mGy and 4.5 mSv, respectively. CT volume-rendered reconstruction (A, B) and conventional angiogram (D, E) show significant stenosis of proximal left anterior descending artery (black arrows) and diagonal branch (white arrows). Radiologist well detected these lesions and they were mentioned on radiologic report. At same time, total segmental occlusion of distal left circumflex artery (arrowheads) was noted (B, E). Mixed plaque occluding lumen of left circumflex artery (white arrowheads) was well depicted on curved multiplanar reconstruction (F). However, in clinical practice, there was no mention of this on radiologic report. Unenhanced left circumflex artery (white arrowhead) is slightly enlarged and it may have been missed since it looks like cardiac vein on axial transverse image (C).
Cited by 1 articles
-
Coronary Computed Tomography Angiography for the Diagnosis of Vasospastic Angina: Comparison with Invasive Coronary Angiography and Ergonovine Provocation Test
Jiesuck Park, Hyung-Kwan Kim, Eun-Ah Park, Jun-Bean Park, Seung-Pyo Lee, Whal Lee, Yong-Jin Kim, Dae-Won Sohn
Korean J Radiol. 2019;20(5):719-728. doi: 10.3348/kjr.2018.0847.
Reference
-
1. Achenbach S, Ropers D, Kuettner A, Flohr T, Ohnesorge B, Bruder H, et al. Contrast-enhanced coronary artery visualization by dual-source computed tomography--initial experience. Eur J Radiol. 2006. 57:331–335.2. Johnson TR, Nikolaou K, Wintersperger BJ, Leber AW, von Ziegler F, Rist C, et al. Dual-source CT cardiac imaging: initial experience. Eur Radiol. 2006. 16:1409–1415.3. Scheffel H, Alkadhi H, Plass A, Vachenauer R, Desbiolles L, Gaemperli O, et al. Accuracy of dual-source CT coronary angiography: first experience in a high pre-test probability population without heart rate control. Eur Radiol. 2006. 16:2739–2747.4. Burgstahler C, Reimann A, Drosch T, Heuschmid M, Brodoefel H, Tsiflikas I, et al. Cardiac dual-source computed tomography in patients with severe coronary calcifications and a high prevalence of coronary artery disease. J Cardiovasc Comput Tomogr. 2007. 1:143–151.5. Heuschmid M, Burgstahler C, Reimann A, Brodoefel H, Mysal I, Haeberle E, et al. Usefulness of noninvasive cardiac imaging using dual-source computed tomography in an unselected population with high prevalence of coronary artery disease. Am J Cardiol. 2007. 100:587–592.6. Johnson TR, Nikolaou K, Busch S, Leber AW, Becker A, Wintersperger BJ, et al. Diagnostic accuracy of dual-source computed tomography in the diagnosis of coronary artery disease. Invest Radiol. 2007. 42:684–691.7. Leber AW, Johnson T, Becker A, von Ziegler F, Tittus J, Nikolaou K, et al. Diagnostic accuracy of dual-source multi-slice CT-coronary angiography in patients with an intermediate pretest likelihood for coronary artery disease. Eur Heart J. 2007. 28:2354–2360.8. Oncel D, Oncel G, Tastan A. Effectiveness of dual-source CT coronary angiography for the evaluation of coronary artery disease in patients with atrial fibrillation: initial experience. Radiology. 2007. 245:703–711.9. Ropers U, Ropers D, Pflederer T, Anders K, Kuettner A, Stilianakis NI, et al. Influence of heart rate on the diagnostic accuracy of dual-source computed tomography coronary angiography. J Am Coll Cardiol. 2007. 50:2393–2398.10. Brodoefel H, Burgstahler C, Tsiflikas I, Reimann A, Schroeder S, Claussen CD, et al. Dual-source CT: effect of heart rate, heart rate variability, and calcification on image quality and diagnostic accuracy. Radiology. 2008. 247:346–355.11. Donnino R, Jacobs JE, Doshi JV, Hecht EM, Kim DC, Babb JS, et al. Dual-source versus single-source cardiac CT angiography: comparison of diagnostic image quality. AJR Am J Roentgenol. 2009. 192:1051–1056.12. Fang XM, Chen HW, Hu XY, Bao J, Chen Y, Yang ZY, et al. Dual-source CT coronary angiography without heart rate or rhythm control in comparison with conventional coronary angiography. Int J Cardiovasc Imaging. 2010. 26:323–331.13. Meng L, Cui L, Cheng Y, Wu X, Tang Y, Wang Y, et al. Effect of heart rate and coronary calcification on the diagnostic accuracy of the dual-source CT coronary angiography in patients with suspected coronary artery disease. Korean J Radiol. 2009. 10:347–354.14. Rixe J, Rolf A, Conradi G, Moellmann H, Nef H, Neumann T, et al. Detection of relevant coronary artery disease using dual-source computed tomography in a high probability patient series: comparison with invasive angiography. Circ J. 2009. 73:316–322.15. Tsiflikas I, Brodoefel H, Reimann AJ, Thomas C, Ketelsen D, Schroeder S, et al. Coronary CT angiography with dual source computed tomography in 170 patients. Eur J Radiol. 2010. 74:161–165.16. Weustink AC, Neefjes LA, Kyrzopoulos S, van Straten M, Neoh Eu R, Meijboom WB, et al. Impact of heart rate frequency and variability on radiation exposure, image quality, and diagnostic performance in dual-source spiral CT coronary angiography. Radiology. 2009. 253:672–680.17. Flohr TG, McCollough CH, Bruder H, Petersilka M, Gruber K, Suss C, et al. First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol. 2006. 16:256–268.18. Burgstahler C, Reimann A, Brodoefel H, Daferner U, Herberts T, Tsiflikas I, et al. Quantitative parameters to compare image quality of non-invasive coronary angiography with 16-slice, 64-slice and dual-source computed tomography. Eur Radiol. 2009. 19:584–590.19. McCollough CH, Primak AN, Saba O, Bruder H, Stierstorfer K, Raupach R, et al. Dose performance of a 64-channel dual-source CT scanner. Radiology. 2007. 243:775–784.20. Stolzmann P, Scheffel H, Schertler T, Frauenfelder T, Leschka S, Husmann L, et al. Radiation dose estimates in dual-source computed tomography coronary angiography. Eur Radiol. 2008. 18:592–599.21. Weustink AC, Mollet NR, Pugliese F, Meijboom WB, Nieman K, Heijenbrok-Kal MH, et al. Optimal electrocardiographic pulsing windows and heart rate: effect on image quality and radiation exposure at dual-source coronary CT angiography. Radiology. 2008. 248:792–798.22. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975. 51:5–40.23. Gouya H, Varenne O, Trinquart L, Touze E, Vignaux O, Spaulding C, et al. Coronary artery stenosis in high-risk patients: 64-section CT and coronary angiography--prospective study and analysis of discordance. Radiology. 2009. 252:377–385.24. Hamon M, Morello R, Riddell JW. Coronary arteries: diagnostic performance of 16- versus 64-section spiral CT compared with invasive coronary angiography--meta-analysis. Radiology. 2007. 245:720–731.25. Wang Y, Vidan E, Bergman GW. Cardiac motion of coronary arteries: variability in the rest period and implications for coronary MR angiography. Radiology. 1999. 213:751–758.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Radiation Dose and Image Quality between the 2nd Generation and 3rd Generation Dual-Source Single-Energy and Dual-Source Dual-Energy CT of the Abdomen
- Pediatric 16-slice CT Protocols: Radiation Dose and Image Quality
- Initial Clinical Experience With Coronary CT Angiography Performed on Dual Source Photon Counting CT Using Different Cardiac Scan Modes-Analysis of Image Quality and Radiation Dose
- A study on radiation exposure dose at brain CT
- Radiation Dose and Imaging Quality of Abdominal Computed Tomography before and after Scan Protocol Adjustment: Single-Institution Experience in Three Years
