Korean J Ophthalmol.
2012 Feb;26(1):61-64. 10.3341/kjo.2012.26.1.61.
Resolution of Recalcitrant Uveitic Optic Disc Edema Following Administration of Methotrexate: Two Case Reports
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. sejoon1@snu.ac.kr
- 2Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- KMID: 1120185
- DOI: http://doi.org/10.3341/kjo.2012.26.1.61
Abstract
- A 13-year-old male and a 15-year-old female presented with optic disc edema associated with chronic recurrent uveitis. While the ocular inflammation responded to high doses of oral prednisolone, the disc edema showed little improvement. After oral administration of methotrexate, the disc edema and ocular inflammation were resolved, and the dose of oral corticosteroid could be reduced.
Keyword
MeSH Terms
Figure
-
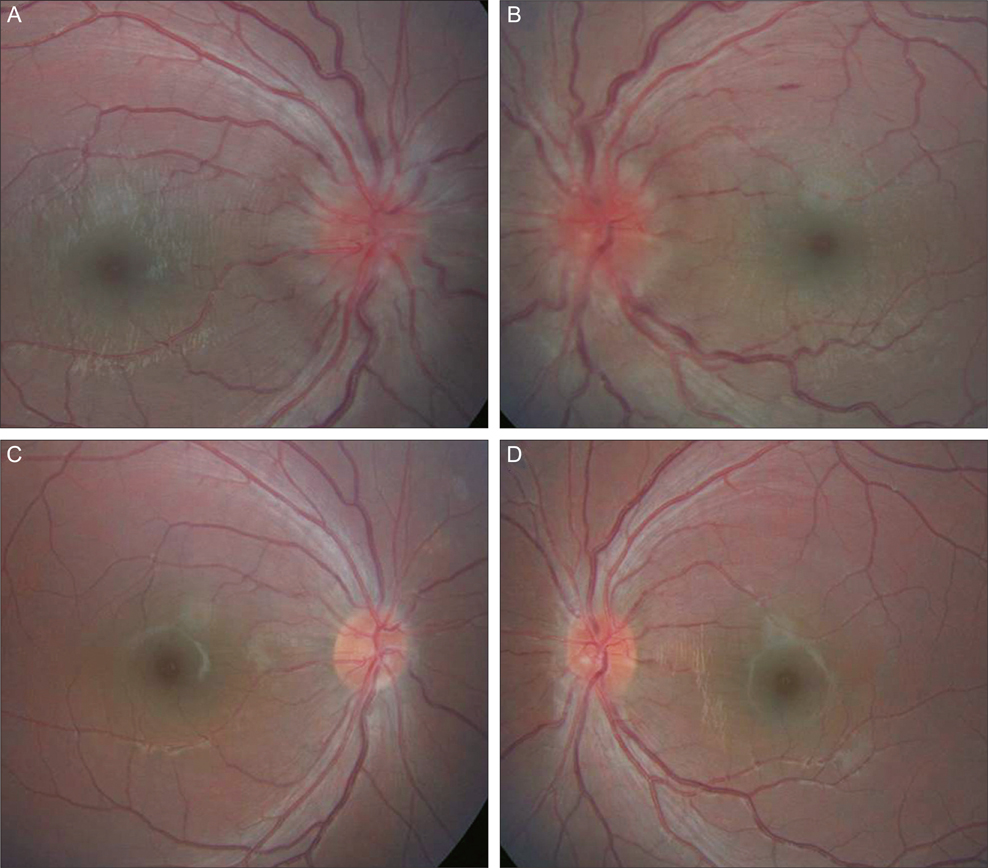
Fig. 1 Case 1. Fundus photographs of case 1. (A,B) At presentation, bilateral severe disc edema and vascular tortuosity were observed. (C,D) Three weeks after administration of methotrexate, disc edema and vascular tortuosity were resolved.
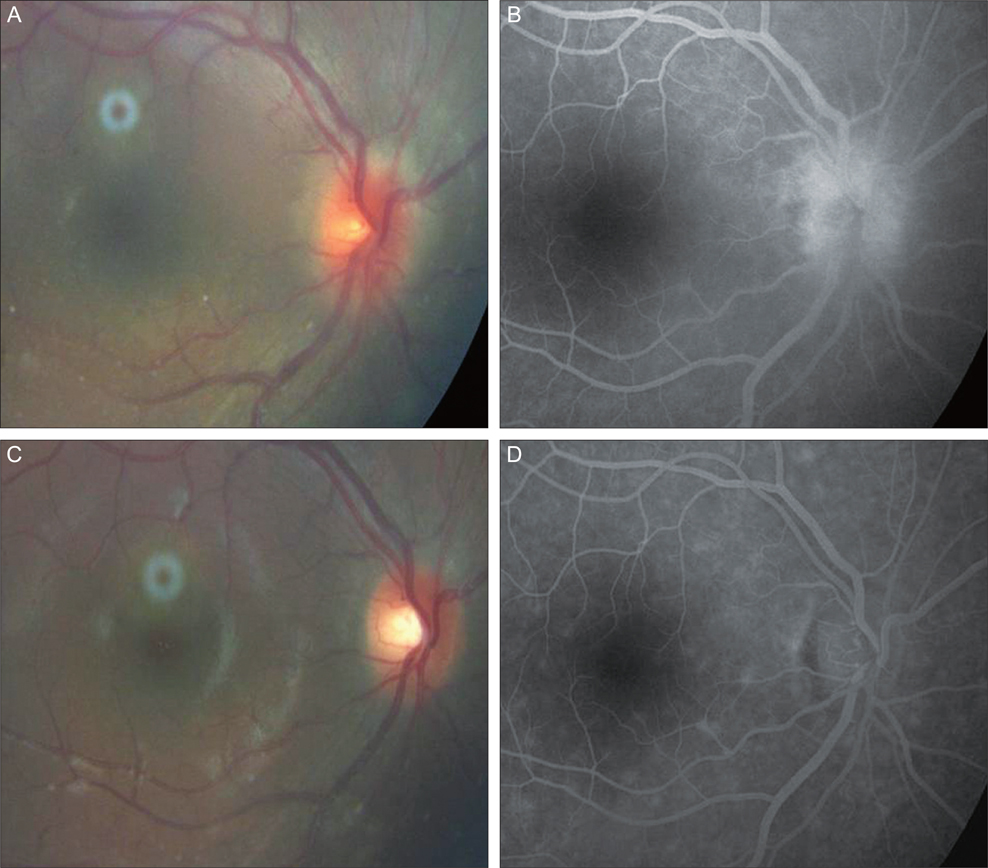
Fig. 2 Case 2. A fundus photograph (A) and fluorescein angiography (B) of the right eye revealing disc edema and choroiditis. (C,D). One month after administration of methotrexate, the disc edema and fluorescein leakage from the optic disc were resolved.
Reference
-
1. Holland GN, Denove CS, Yu F. Chronic anterior uveitis in children: clinical characteristics and complications. Am J Ophthalmol. 2009. 147:667–678.2. Kozak I, Robbins SL, Freeman WR. Bilateral papillitis associated with bilateral anterior uveitis in a child. J Pediatr Ophthalmol Strabismus. 2007. 44:374–376.3. Gangaputra S, Newcomb CW, Liesegang TL, et al. Methotrexate for ocular inflammatory diseases. Ophthalmology. 2009. 116:2188–2198.4. Rebolleda G, Mu?oz-Negrete FJ. Follow-up of mild papilledema in idiopathic intracranial hypertension with optical coherence tomography. Invest Ophthalmol Vis Sci. 2009. 50:5197–5200.5. Monheit BE, Read RW. Optic disk edema associated with sudden-onset anterior uveitis. Am J Ophthalmol. 2005. 140:733–735.6. Foeldvari I, Wierk A. Methotrexate is an effective treatment for chronic uveitis associated with juvenile idiopathic arthritis. J Rheumatol. 2005. 32:362–365.7. Malik AR, Pavesio C. The use of low dose methotrexate in children with chronic anterior and intermediate uveitis. Br J Ophthalmol. 2005. 89:806–808.8. Walker AM, Funch D, Dreyer NA, et al. Determinants of serious liver disease among patients receiving low-dose methotrexate for rheumatoid arthritis. Arthritis Rheum. 1993. 36:329–335.9. Hoekstra M, van Ede AE AE, Haagsma CJ, et al. Factors associated with toxicity, final dose, and efficacy of methotrexate in patients with rheumatoid arthritis. Ann Rheum Dis. 2003. 62:423–426.10. Van Ede AE, Laan RF, Blom HJ, et al. Methotrexate in rheumatoid arthritis: an update with focus on mechanisms involved in toxicity. Semin Arthritis Rheum. 1998. 27:277–292.11. Salaffi F, Manganelli P, Carotti M, et al. Methotrexate-induced pneumonitis in patients with rheumatoid arthritis and psoriatic arthritis: report of five cases and review of the literature. Clin Rheumatol. 1997. 16:296–304.12. Ohosone Y, Okano Y, Kameda H, et al. Toxicity of low-dose methotrexate in rheumatoid arthritis: clinical characteristics in patients with MTX-induced pancytopenia and interstitial pneumonitis. Ryumachi. 1997. 37:16–23.13. Doroshow JH, Locker GY, Gaasterland DE, et al. Ocular irritation from high-dose methotrexate therapy: pharmacokinetics of drug in the tear film. Cancer. 1981. 48:2158–2162.14. Johansson BA. Visual field defects during low-dose methotrexate therapy. Doc Ophthalmol. 1992. 79:91–94.15. Balachandran C, McCluskey PJ, Champion GD, Halmagyi GM. Methotrexate-induced optic neuropathy. Clin Experiment Ophthalmol. 2002. 30:440–441.16. Clare G, Colley S, Kennett R, Elston JS. Reversible optic neuropathy associated with low-dose methotrexate therapy. J Neuroophthalmol. 2005. 25:109–112.17. Sbeity ZH, Baydoun L, Schmidt S, Loeffler KU. Visual field changes in methotrexate therapy. Case report and review of the literature. J Med Liban. 2006. 54:164–167.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Optic Disc Appearance in Anterior ischemic optic neuropathy and Optic neuritis
- A Case of Recalcitrant Psoriasis Improved with Tacrolimus (FK 506)
- Hypertensive Optic Neuropathy Related to Chorioretinal Lesions
- A Case of Optic Disc Pit
- Leukemic Infiltration of the Optic Nerve Head: A Case Report
