Retroperitoneal Malignant Mesenchymoma: A Case of Mesenchymal Mixed Tumor with Osteosarcoma, Leiomyosarcoma, Liposarcoma and Fibrosarcoma
- Affiliations
-
- 1Department of Radiology, Holy Family Hospital, The Catholic University of Korea, Korea. hjchung@hfh.cuk.ac.kr
- 2Department of General Surgery, Holy Family Hospital, The Catholic University of Korea, Korea.
- 3Department of Pathology, Holy Family Hospital, The Catholic University of Korea, Korea.
- KMID: 1118795
- DOI: http://doi.org/10.3348/kjr.2002.3.4.264
Abstract
- Malignant mesenchymoma is an interesting but very rare tumor in which malignant differentiation has occurred twice or more. We report a case of retroperitoneal malignant mesenchymoma consisting of osteosarcoma, leiomyosarcoma, liposarcoma and fibrosarcoma. Abdominal CT showed a large retroperitoneal mass with two separate and distinct parts, namely an area of prominent calcification and one of clearly enhancing solid components. The mass contained histologically distinct tumorous components with no histologic admixure at the interfaces. The densely calcified nodule corresponded to osteosarcoma, and the noncalcified clearly enhancing nodules to leiomyosarcoma, liposarcoma and fibrosarcoma.
Keyword
MeSH Terms
Figure
-
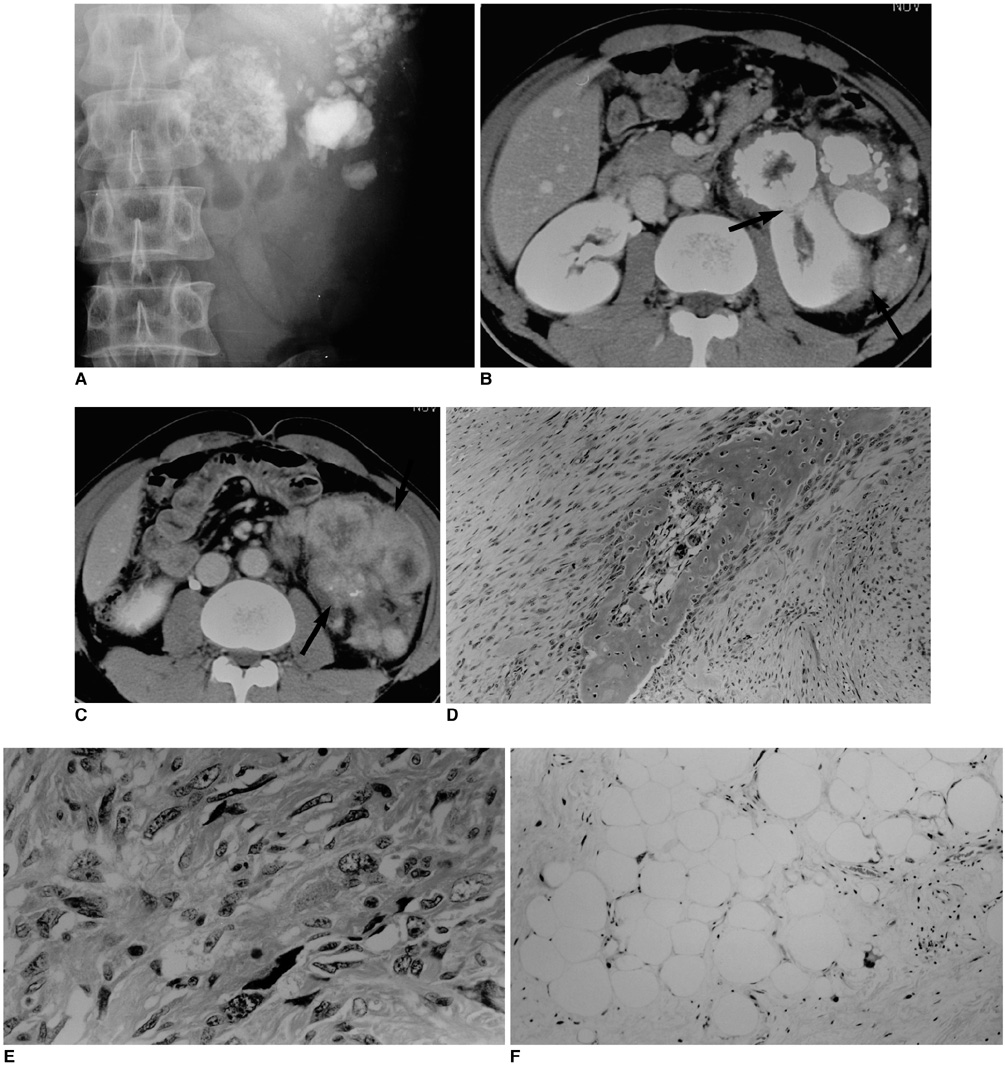
Fig. 1 A 47-year-old man with retroperitoneal malignant mesenchymoma. A. Plain abdominal radiograph demonstrates a large mass with multiple, dense, large, stippled calcifications in the left-side abdomen. B. Contrast-enhanced abdominal CT scan at the renal level depicts a large conglomerate mass with densely calcified nodules, shown at histopathologic correlation to be consistent with osteosarcoma, in the left-side reteroperitoneum. The mass invades the left kidney (arrows). C. Contrast-enhanced abdominal CT scan, caudal to that seen in (B), depicts lobulated non-calcified soft tissue nodules (arrows) with strong peripheral enhancement and, in some areas, central low attenuation. The nodules correspond to leiomyosarcoma, liposarcoma, and fibrosarcoma. D. Microscopically, the osteosarcomatous component consists of a central malignant osteoid within a background of malignant spindle cells (original magnification, ×100; hematoxylin-eosin staining). E. Microscopically, the leiomyosarcomatous component contains typical blunt-ended nuclei with mitotic configuration (original magnification, ×100; hematoxylin-eosin staining). F. Microscopically, the liposarcomatous component contains occasional scattered lipoblasts between fat cells (original magnification, ×100; hematoxylin-eosin staining).
Cited by 1 articles
-
Retroperitoneal Extraskeletal Osteosarcoma without Calcification Mimicking Pancreas Tumor: CT Imaging of a Case Report
Jung Won Kim, Kyung Eun Bae, Kyeong Mee Park, Jae Hyung Kim, Myeong Ja Jeong, Soung Hee Kim, Ji Young Kim, Soo Hyun Kim, Mi Jin Kang, Ji Hae Lee, Tae Gyu Kim
J Korean Soc Radiol. 2018;78(5):340-344. doi: 10.3348/jksr.2018.78.5.340.
Reference
-
1. Stout AP. Mesenchymoma, the mixed tumor of mesenchymal derivatives. Ann Surg. 1948. 127:278–290.2. Fujiyoshi Y, Nishimura H, Irie K, et al. A case of retroperitoneal malignant mesenchymoma. Pathol Int. 1994. 44:803–807.3. Satake I, Tari K, Nakagomi K, et al. Retroperitoneal malignant mesenchymoma: a case report. Int J Urol. 1994. 1:273–274.4. Mukherji SK, Rojiani AM, Younathan CM, et al. CT findings of retroperitoneal malignant mesenchymoma. Abdom Imaging. 1994. 19:82–83.5. Suzuki S, Furui S, Kokubo T, et al. Retroperitoneal malignant mesenchymoma: imaging findings in five cases. Abdom Imaging. 1999. 24:92–97.6. Brady MS, Perino G, Tallini G, et al. Malignant mesenchymoma. Cancer. 1996. 77:467–473.7. Newman PL, Fletcher CDM. Malignant mesenchymoma. clinicopathologic analysis of a series with evidence of low-grade behavior. Am J Surg Pathol. 1991. 15:607–614.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Malignant Mesenchymoma in Inguinal Region
- Malignant Mesenchymoma of the Right Axillary Area: A case report
- Malignant Mixed Mesodermal Tumor of the Urinary Bladder: A Case Report and Literature Review
- Two cases of Benign Mesenchymoma arising in Thigh and Forearm
- Malignant Mixed Mullerian Tumor of Fallopian Tube with Multiple Distinct Heterologous Components
