A Case of Retained Graphite Anterior Chamber Foreign Body Masquerading as Stromal Keratitis
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea. jyhyon@snu.ac.kr
- 2Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- KMID: 1111875
- DOI: http://doi.org/10.3341/kjo.2011.25.2.128
Abstract
- We report a case of a retained graphite anterior chamber foreign body that was masquerading as stromal keratitis. A 28-year-old male visited with complaints of visual disturbance and hyperemia in his right eye for four weeks. On initial examination, he presented with a stromal edema involving the inferior half of the cornea, epithelial microcysts, and moderate chamber inflammation. Suspecting herpetic stromal keratitis, he was treated with anti-viral and anti-inflammatory agents. One month after the initial visit, anterior chamber inflammation was improved and his visual acuity recovered to 20/20, but subtle corneal edema still remained. On tapering the medication, after three months, a foreign body was incidentally identified in the inferior chamber angle and was surgically removed resulting in complete resolution of corneal edema. The removed foreign body was a fragment of graphite and he subsequently disclosed a trauma with mechanical pencil 12 years earlier. This case showed that the presence of an anterior chamber foreign body should always be considered in the differential diagnosis of idiopathic localized corneal edema.
Keyword
MeSH Terms
Figure
-
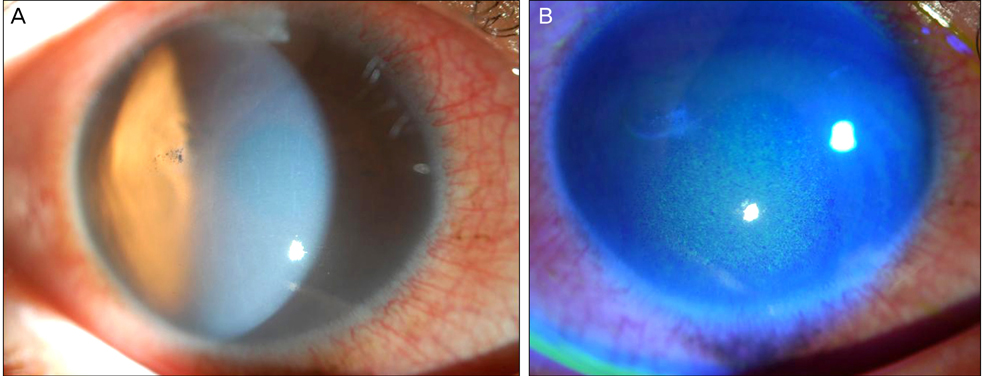
Fig. 1 A slit lamp biomicroscopic finding on the patient's initial visit revealed conjunctival hyperemia, localized corneal stromal edema with epithelial microcysts, and moderate chamber inflammation. A focal mid-stromal scar at the temporal cornea was also noted.

Fig. 2 After five days of steroid treatment, stromal edema was decreased and the patient's vision improved to 20/20. Localized epithelial microcysts were still observed.
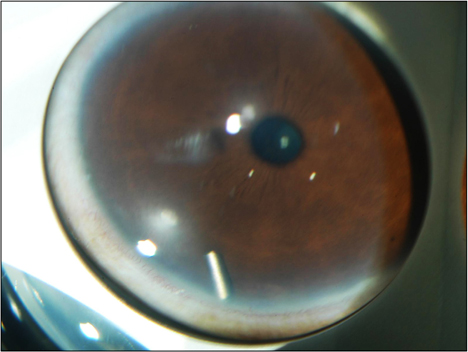
Fig. 3 At three months after initial visit, a previously unobserved foreign body was incidentally identified in the inferior angle of anterior chamber.

Fig. 4 Removed anterior chamber foreign body measuring about 0.5×1.5 mm in size.
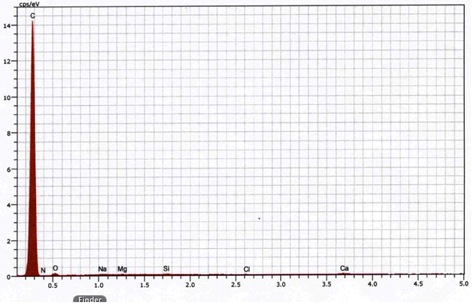
Fig. 5 Energy dispersive X-ray spectroscopy of the removed foreign body revealed that it contains mainly elementary carbons, which implies that the foreign body is a broken graphite pencil lead.
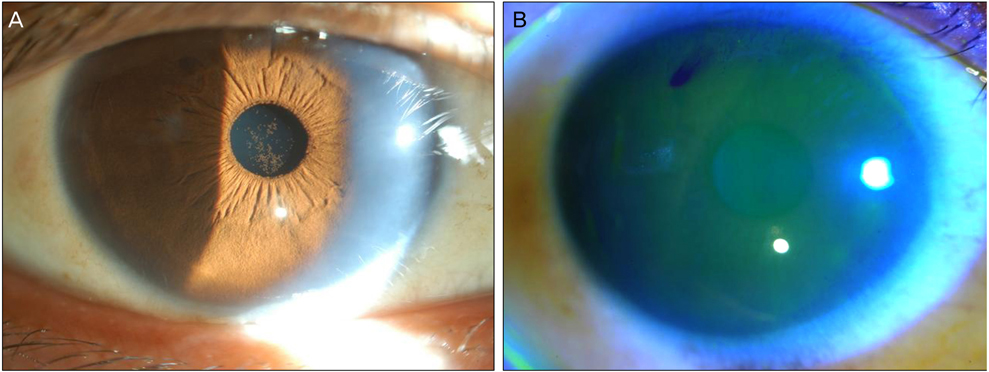
Fig. 6 Two weeks after removal of the foreign body, the previous corneal stromal edema and epithelial microcysts were completely resolved.
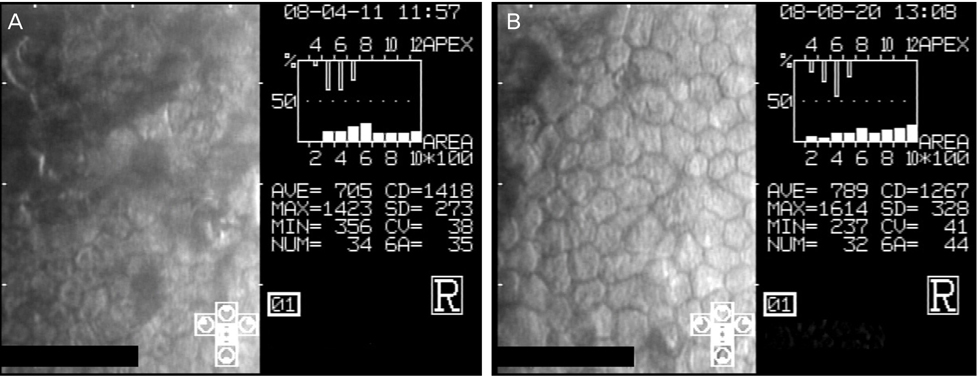
Fig. 7 Specular microscopy findings before (A) and two weeks after (B) the surgery. Corneal endothelial cell density reduced following the episode of corneal edema, but the percentage of hexagonal cells improved from 35% to 44% after removal of the foreign body. APEX = apex; AVE = average; MAX = maximum; MIN = minimum; NUM = number; CD = cell density; SD = standard deviation; CV = coefficient of variation; 6A = hexagonality.
Reference
-
1. Archer DB, Davies MS, Kanski JJ. Non-metallic foreign bodies in the anterior chamber. Br J Ophthalmol. 1969. 53:453–456.2. Kim JH, Park KS. A case of eye lashes in an anterior chamber. J Korean Ophthalmol Soc. 1968. 9:23–25.3. Chang YS, Jeong YC, Ko BY. A case of an asymptomatic intralenticular foreign body. Korean J Ophthalmol. 2008. 22:272–275.4. Kargi SH, Oz O, Erdinc E, et al. Tolerated cilium in the anterior chamber. Ocul Immunol Inflamm. 2003. 11:73–78.5. Stangos AN, Pournaras CJ, Petropoulos IK. Occult anterior-chamber metallic fragment post-phacoemulsification masquerading as chronic recalcitrant postoperative inflammation. Am J Ophthalmol. 2005. 139:541–542.6. Brown SI. Corneal edema from a cotton foreign body in the anterior chamber. Am J Ophthalmol. 1968. 65:616–617.7. Honda Y, Asayama K. Intraocular graphite pencil lead without reaction. Am J Ophthalmol. 1985. 99:494–495.8. Hamanaka N, Ikeda T, Inokuchi N, et al. A case of an intraocular foreign body due to graphite pencil lead complicated by endophthalmitis. Ophthalmic Surg Lasers. 1999. 30:229–231.9. Guy JR, Rao NA. Graphite foreign body of the conjunctiva simulating melanoma. Cornea. 1985-1986. 4:263–265.10. Jeng BH, Whitcher JP, Margolis TP. Intracorneal graphite particles. Cornea. 2004. 23:319–320.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noninfectious Endophthalmitis Caused by an Intraocular Foreign Body Retained for 16 Years
- A Case of Graphite Foreign Body Misdiagnosed as Blue Nevus
- Keratitis Treatment by Removal of Concealed Retrocorneal Plant Foreign Body
- Intraocular Foreign Body of a Vitreous Cutter Tip Fragment
- A Case of Eye Lashes in an Anterior Chamber
