Yonsei Med J.
2011 Jan;52(1):199-203. 10.3349/ymj.2011.52.1.199.
Solitary Extrahepatic Intraabdominal Metastasis from Hepatocellular Carcinoma after Liver Transplantation
- Affiliations
-
- 1Department of Surgery, Korea University College of Medicine, Seoul, Korea.
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. kskim88@yuhs.ac
- KMID: 1106458
- DOI: http://doi.org/10.3349/ymj.2011.52.1.199
Abstract
- A liver transplantation is a treatment option in selected patients with hepatocellular carcinoma (HCC). Despite the adequate selection of candidates, recurrences of HCC may still develop. Solitary extrahepatic metastasis from HCC after a liver transplantation is rare. Here we report two cases of HCC demonstrated extrahepatic recurrence to the adrenal gland and spleen, respectively, within one year after a liver transplantation. Since the treatment of solitary extrahepatic metastasis from HCC after a liver transplantation is not standardized, surgical resection was performed. In the case of HCC adrenal metastasis, innumerable intrahepatic metastases were found two months after the adrenalectomy. And 16 months after adrenalectomy, the patient expired due to tumor progression and hepatic failure. In the case of HCC splenic metastasis, postoperative radiation therapy was performed. However, two recurrent HCC nodules were found 15 months after the splenectomy and received transarterial chemoembolization (TACE). And 29 month after the splenectomy, the patient also expired as same causes of former patient.
MeSH Terms
Figure
-
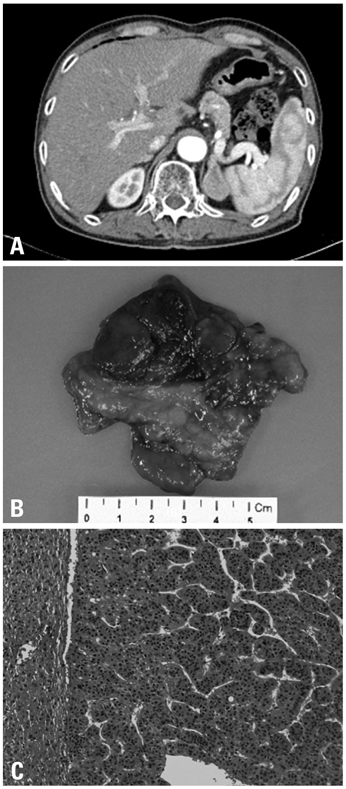
Fig. 1 A CT scan reveals a newly-developed solitary left adrenal mass, which was 3.5 × 2.3 cm in size, homogenous, and well-demarcated, suggesting HCC metastasis (A). Pathologic specimen following adrenalectomy (B) and microscopic exam, Hematoxylin & Eosin stain, ×100 (C).
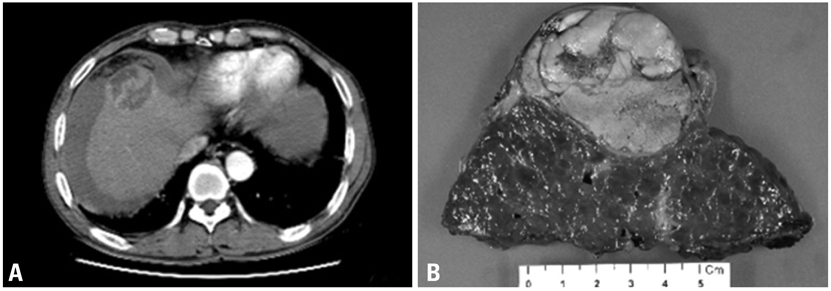
Fig. 2 A CT scan demonstrates a ruptured HCC located in segment VIII of the liver (A). Central bisectionectomy was performed following TACE, and the mass was a 5.7 cm HCC with 60% necrosis (B). HCC, hepatocellular carcinoma.
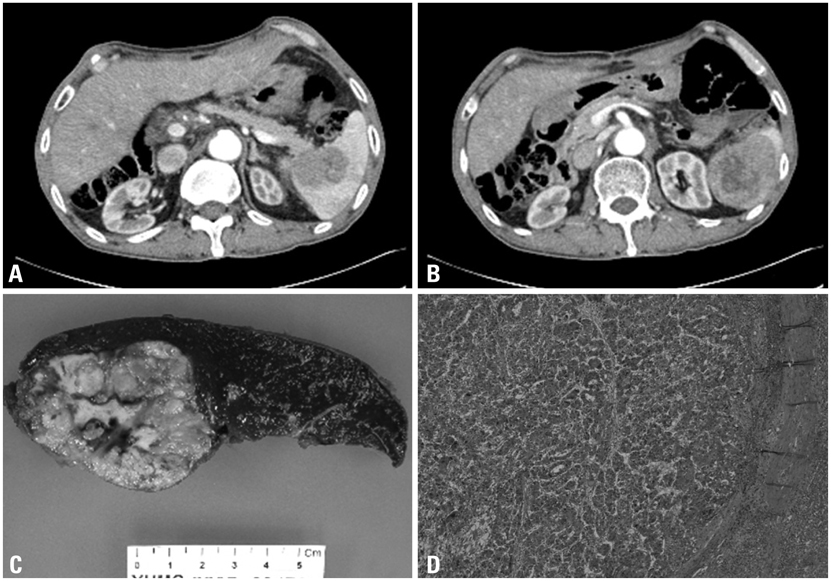
Fig. 3 A newly-developed, 3 cm-sized heterogeneous mass was found in the hilum of the spleen after liver transplantation (A and B). Pathologic specimen following splenectomy (C) and microscopic exam, Hematoxylin & Eosin stain, ×40 (D).
Reference
-
1. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996. 334:693–699.
Article2. Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001. 33:1394–1403.
Article3. Schwartz M. Liver transplantation for hepatocellular carcinoma. Gastroenterology. 2004. 127:5 Suppl 1. S268–S276.
Article4. Katyal S, Oliver JH 3rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carcinoma. Radiology. 2000. 216:698–703.
Article5. Castroagudín JF, González-Quintela A, Martínez J, Tomé S, Forteza J, Varo E. Bilateral adrenal metastases from hepatocellular carcinoma after liver transplantation. Hepatogastroenterology. 2002. 49:249–251.6. Nakashima T, Okuda K, Kojiro M, Jimi A, Yamaguchi R, Sakamoto K, et al. Pathology of hepatocellular carcinoma in Japan. 232 Consecutive cases autopsied in ten years. Cancer. 1983. 51:863–877.
Article7. Hu RH, Ho MC, Wu YM, Yu SC, Lee PH. Feasibility of salvage liver transplantation for patients with recurrent hepatocellular carcinoma. Clin Transplant. 2005. 19:175–180.
Article8. Llovet J, Schwartz M, Mazzaferro V. Resection and liver transplantation for hepatocellular carcinoma. Semin Liver Dis. 2005. 25:181–200.
Article9. Pérez-Saborido B, de los Galanes SJ, Menéu-Díaz JC, Romero CJ, Elola-Olaso AM, Suárez YF, et al. Tumor recurrence after liver transplantation for hepatocellular carcinoma: recurrence pathway and prognostic factors. Transplant Proc. 2007. 39:2304–2307.
Article10. Vivarelli M, Cucchetti A, Piscaglia F, La Barba G, Bolondi L, Cavallari A, et al. Analysis of risk factors for tumor recurrence after liver transplantation for hepatocellular carcinoma: key role of immunosuppression. Liver Transpl. 2005. 11:497–503.
Article11. Escartin A, Sapisochin G, Bilbao I, Vilallonga R, Bueno J, Castells L, et al. Recurrence of hepatocellular carcinoma after liver transplantation. Transplant Proc. 2007. 39:2308–2310.
Article12. Poon RT, Fan ST, O'uilleabhain CB, Wong J. Aggressive management of patients with extrahepatic and intrahepatic recurrences of hepatocellular carcinoma by combined resection and locoregional therapy. J Am Coll Surg. 2002. 195:311–318.
Article13. Seong J. Challenge and hope in radiotherapy of hepatocellular carcinoma. Yonsei Med J. 2009. 50:601–612.
Article14. Park JS, Yoon DS, Kim KS, Choi JS, Lee WJ, Chi HS, et al. What is the best treatment modality for adrenal metastasis from hepatocellular carcinoma? J Surg Oncol. 2007. 96:32–36.
Article15. Lee SS, Morgenstern L, Phillips EH, Hiatt JR, Margulies DR. Splenectomy for splenic metastases: a changing clinical spectrum. Am Surg. 2000. 66:837–840.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Extrahepatic Metastasis of Hepatocellular Carcinoma to the Pronator Quadratus Muscle of Right Wrist
- Transarterial Chemoembolization in Patients with Hepatocellular Carcinoma and Extrahepatic Metastasis
- Uptake of 99mTc - DISDA in Primary Hepatocellular Carcinoma and Metastatic Nodule in the Lung
- Solitary Paraaortic Lymph Node Metastasis of Primary Hepatocellular Carcinoma which was Misdiagnosed as Primary Retroperitoneal Tumor
- A case of hepatocellular carcinoma combined with solitary parathyroid metastasis
