Balloon Sheaths for Gastrointestinal Guidance and Access: A Preliminary Phantom Study
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Korea. jhshin@amc.seoul.kr
- 2Department of Radiology, Nanjing First Hospital, Nanjing Medical University.
- 3Department of Information and Statistics, Daejeon University, Korea.
- KMID: 1102713
- DOI: http://doi.org/10.3348/kjr.2005.6.3.167
Abstract
OBJECTIVE
We wanted to evaluate the feasibility and usefulness of a newly designed balloon sheath for gastrointestinal guidance and access by conducting a phantom study. MATERIALS AND METHODS: The newly designed balloon sheath consisted of an introducer sheath and a supporting balloon. A coil catheter was advanced over a guide wire into two gastroduodenal phantoms (one was with stricture and one was without stricture) ; group I was without a balloon sheath, group ll was with a deflated balloon sheath, and groups III and IV were with an inflated balloon and with the balloon in the fundus and body, respectively. Each test was performed for 2 minutes and it was repeated 10 times in each group by two researchers, and the positions reached by the catheter tip were recorded. RESULTS: Both researchers had better performances with both phantoms in order of group IV, III, II and I. In group IV, both researchers advanced the catheter tip through the fourth duodenal segment in both the phantoms. In group I, however, the catheter tip never reached the third duodenal segment in both the phantoms by both the researchers. The numeric values for the four study groups were significantly different for both the phantoms (p < 0.001). A significant difference was also found between group III and IV for both phantoms (p < 0.001). CONCLUSION: The balloon sheath seems to be feasible for clinical use, and it has good clinical potential for gastrointestinal guidance and access, particularly when the inflated balloon is placed in the gastric body.
MeSH Terms
Figure
-
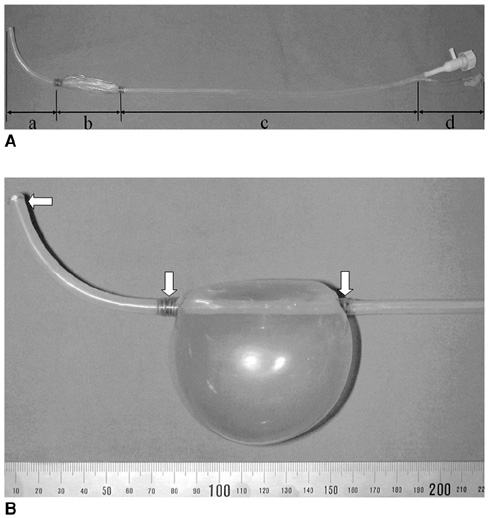
Fig. 1 The new balloon sheath. A. The deflated balloon sheath. (a) the distal angulated part, (b) the balloon part, (c) the straight part, and (d) the proximal handling part. B. The inflated balloon sheath and the three gold markers (arrows) at each end of the balloon and at the tip of the balloon sheath.
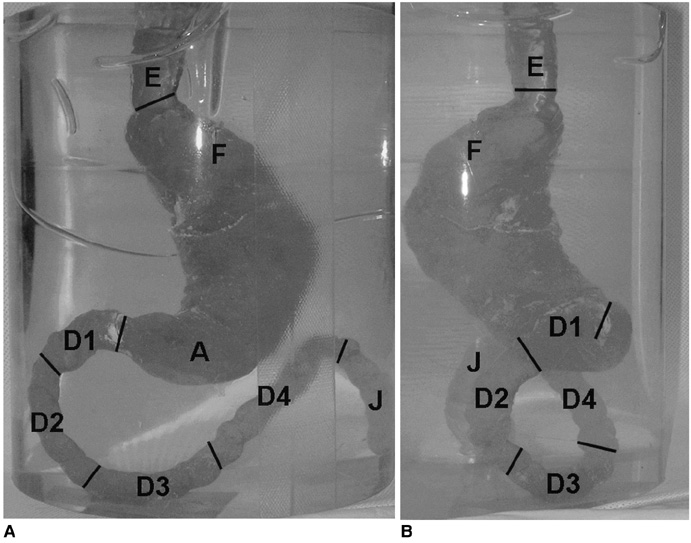
Fig. 2 Photograph of the silicone phantom model without stricture and filled with red ink. A. Anteroposterior view. B. Lateral view. The gastroduodenal junction is angled about 90° in a posterior direction to the long axis of the gastric antrum. E = esophagus, F = fundus, A = antrum, D1 = first segment of duodenum, D2 = second segment of duodenum, D3 = third segment of duodenum, D4 = fourth segment of duodenum, J = proximal portion of the jejunum.
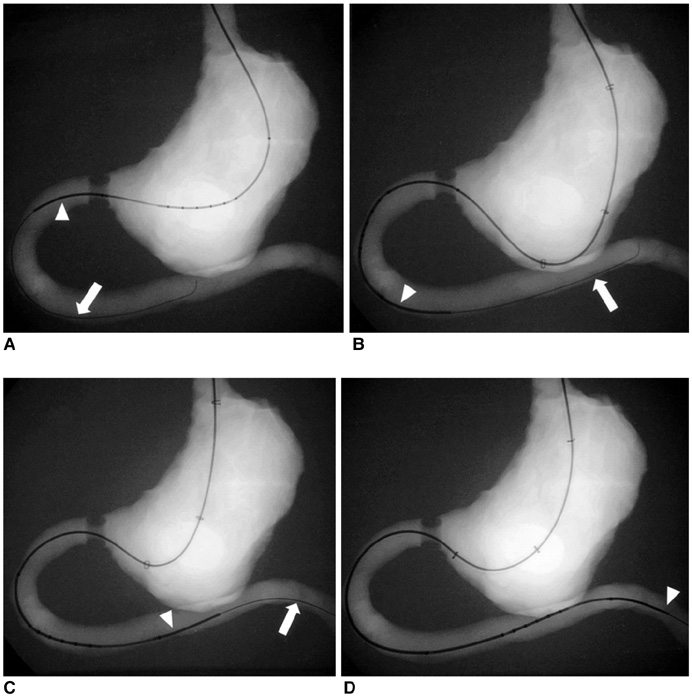
Fig. 3 Radiographies of a coil catheter (arrowheads) being advanced over a guide wire (arrows) into the gastroduodenal phantom with stricture in the four groups. A. Group I, without a balloon sheath. B. Group II, through the deflated balloon sheath. C. Group III, through the inflated balloon sheath with the inflated balloon located in the gastric fundus. D. Group IV, through the inflated balloon sheath with the inflated balloon located in the gastric body.
Reference
-
1. Jung GS, Song HY, Kang SG, Huh JD, Park SJ, Koo JY, et al. Malignant gastroduodenal obstructions: treatment by means of a covered expandable metallic stent-initial experience. Radiology. 2000. 216:758–763.2. Mauro MA, Koehler RE, Baron TH. Advances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents. Radiology. 2000. 215:659–669.3. Holt PD, de Lange EE, Shaffer HA Jr. Strictures after gastric surgery: treatment with fluroscopically guided balloon dilation. AJR Am J Roentgenol. 1995. 164:895–899.4. Binkert CA, Jost R, Steiner A, Zollikofer CL. Benign and malignant stenoses of the stomach and duodenum: treatment with self-expanding metallic endoprostheses. Radiology. 1996. 199:335–338.5. Jung GS, Song HY, Seo TS, Park SJ, Koo JY, Huh JD, et al. Malignant gastric outlet obstructions: treatment by means of coaxial placement of uncovered and covered expandable nitinol stents. J Vasc Interv Radiol. 2002. 13:275–283.6. Park KB, Do YS, Kang WK, Choo SW, Han YH, Suh SW, et al. Malignant obstruction of gastric outlet and duodenum: palliation with flexible covered metallic stents. Radiology. 2001. 219:679–683.7. Yates MR 3rd, Morgan DE, Baron TH. Palliation of malignant gastric and small intestinal strictures with self-expandable metal stents. Endoscopy. 1998. 30:266–272.8. Razzaq R, Laasch HU, England R, Marriott A, Martin D. Expandable metal stents for the palliation of malignant gastroduodenal obstruction. Cardiovasc Intervent Radiol. 2001. 24:313–318.9. Caldicott DG, Ziprin P, Morgan R. Transhepatic insertion of a metallic stent for the relief of malignant afferent loop obstruction. Cardiovasc Intervent Radiol. 2000. 23:138–140.10. Lee JM, Han YM, Kim CS, Lee SY, Lee ST, Yang DH. Fluoroscopic-guided covered metallic stent placement for gastric outlet obstruction and post-operative gastroenterostomy anastomotic stricture. Clin Radiol. 2001. 56:560–567.11. Acunas B, Poyanli A, Rozanes I. Intervention in gastrointestinal tract: the treatment of esophageal, gastroduodenal and colorectal obstructions with metallic stents. Eur J Radiol. 2002. 42:240–248.12. Shin JH, He X, Lee JH, Seo TS, Lim JO, Kim TH, et al. Newly designed multifunctional coil catheter for gastrointestinal intervention: feasibility determined by experimental study in dogs. Invest Radiol. 2003. 38:796–801.13. Song HY, Shin JH, Lim JO, Kim TH, Lee GH, Lee SK. Use of a newly designed multifunctional coil catheter for stent placement in the upper gastrointestinal tract. J Vasc Interv Radiol. 2004. 15:369–373.14. Zollikofer CL, Jost R, Schoch E, Decurtins M. Gastrointestinal stenting. Eur Radiol. 2000. 10:329–341.15. Kim JH, Yoo BM, Lee KJ, Hahm KB, Cho SW, Park JJ, et al. Self-expanding coil stent with a long delivery system for palliation of unresectable malignant gastric outlet obstruction: a prospective study. Endoscopy. 2001. 33:838–842.16. Pinto IT. Malignant gastric and duodenal stenosis: palliation by peroral implantation of a self-expanding metallic stent. Cardiovasc Intervent Radiol. 1997. 20:431–434.17. Song HY, Song HY, Shin JH, Lee GH, Kim TW, Lee SK, et al. A dual expandable nitinol stent: experience in 102 patients with malignant gastroduodenal strictures. J Vasc Interv Radiol. 2004. 15:1443–1449.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Newly Designed Sheaths for Gastroduodenal Intervention: An Experimental Study in a Phantom and Dogs
- A Case of Bleeding from a Jejunal Gastrointestinal Stromal Tumor Diagnosed by Double Balloon Enteroscopy
- Balloon Dilatation for Postoperative Stricture of Gastrointestinal Tract
- Volume Measurement Using 3-Dimensional US
- Usefulness of double balloon enteroscopy in obscure gastrointestinal bleeding
