Upper Airway Volume Segmentation Analysis Using Cine MRI Findings in Children with Tracheostomy Tubes
- Affiliations
-
- 1Department of Radiology, Cincinnati Children's Hospital Medical Center, Cincinnati OH, USA. Lane.Donnelly@cchmc.org
- 2Department of Radiology, Emory University School of Medicine, Atlanta GA, USA.
- 3Department of Radiology, University of Arizona College of Medicine, Tucson AZ, USA.
- 4Department of Pediatrics, Cincinnati Children's Hospital Medical Center, Cincinnati OH, USA.
- 5University of Cincinnati, College of Medicine, Cincinnati, OH, USA.
- 6Department of Pulmonary Medicine, Cincinnati Children's Hospital Medical Center, Cincinnati OH, USA.
- 7Department of Otolaryngology, Cincinnati Children's Hospital Medical Center, Cincinnati OH, USA.
- KMID: 1089438
- DOI: http://doi.org/10.3348/kjr.2007.8.6.506
Abstract
- OBJECTIVE: The purpose of this study is to evaluate the airway dynamics of the upper airway as depicted on cine MRI in children with tracheotomy tubes during two states of airflow through the upper airway. MATERIALS AND METHODS: Sagittal fast gradient echo cine MR images of the supra-glottic airway were obtained with a 1.5T MRI scanner on seven children with tracheotomy tubes. Two sets of images were obtained with either the tubes capped or uncapped. The findings of the cine MRI were retrospectively reviewed. Volume segmentation of the cine images to compare the airway volume change over time (mean volume, standard deviation, normalized range, and coefficient of variance) was performed for the capped and uncapped tubes in both the nasopharynx and hypopharynx (Signed Rank Test). RESULTS: Graphical representation of the airway volume over time demonstrates a qualitative increased fluctuation in patients with the tracheotomy tube capped as compared to uncapped in both the nasopharyngeal and hypopharyngeal regions of interest. In the nasopharynx, the mean airway volume (capped 2.72 mL, uncapped 2.09 mL, p = 0.0313), the airway volume standard deviation (capped 0.42 mL, uncapped 0.20 mL, p = 0.0156), and the airway volume range (capped 2.10 mL, uncapped 1.09 mL, p = 0.0156) were significantly larger in the capped group of patients. In the hypopharynx, the airway volume standard deviation (capped 1.54 mL, uncapped 0.67 mL, p = 0.0156), and the airway volume range (capped 6.44 mL, uncapped 2.93 mL, p = 0.0156) were significantly larger in the capped tubes. The coefficient of variance (capped 0.37, uncapped 0.26, p = 0.0469) and the normalized range (capped 1.52, uncapped 1.09, p = 0.0313) were significantly larger in the capped tubes. CONCLUSION: There is a statistically significant change in airway dynamics in children with tracheotomy tubes when breathing via the airway as compared to breathing via the tracheotomy tube.
MeSH Terms
-
Adolescent
Child
Child, Preschool
Female
Humans
Hypopharynx/anatomy & histology/*physiology
Image Processing, Computer-Assisted
Magnetic Resonance Imaging, Cine/*methods
Male
Nasopharynx/anatomy & histology/*physiology
Retrospective Studies
Time Factors
Tracheostomy/*instrumentation
Work of Breathing/*physiology
Figure
-

Fig. 1 Sagittal cine MR images obtained with a 1.5T scanner in an 11-year-old boy with difficulty in tracheotomy tube decannulation, with the tracheotomy tube capped. A. Gradient-recalled-echo cine image. The line shows the region of interest of the nasopharynx. B. Gradient-recalled-echo cine image. The line shows the region of interest of the hypopharynx.
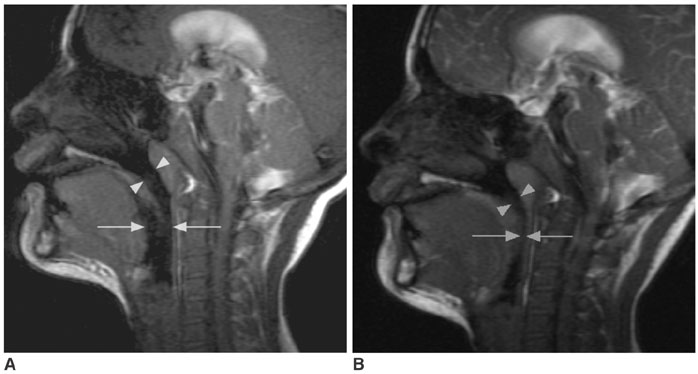
Fig. 2 Sagittal cine MR images obtained with a 1.5T scanner in an 11-year-old boy with difficulty in tracheotomy tube decannulation. A, B. An image obtained with the tracheotomy tube capped (A) shows a larger patent nasopharynx (arrowheads) and hypopharynx (arrows) as compared to the image obtained with the tracheotomy tube uncapped (B).

Fig. 3 Plot of volume versus time of the hypopharynx with the tracheotomy tube capped and uncapped in an 11-year-old boy with difficulty in tracheotomy tube decannulation, displaying increased airway dynamics in the capped series.
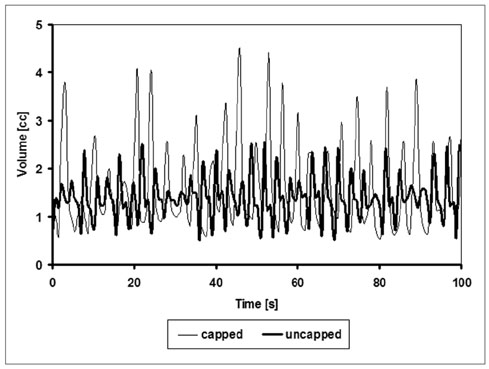
Fig. 4 Plot of volume versus time of the hypopharynx with the tracheotomy tube capped and uncapped in a 9-year-old boy with difficulty in tracheotomy tube decannulation, displaying increased airway dynamics in the capped series, but with a similar mean airway volume.
Reference
-
1. Remmers JE, deGrott WJ, Sauerland EK, Anch AM. Pathogenesis of upper airway occlusion during sleep. J Appl Physiol. 1978. 44:931–938.2. Wilson SL, Thach BT, Brouillette RE, Abu-Osba YK. Upper airway patency in the human infant: influence of airway pressure and posture. J Appl Physiol. 1980. 48:500–504.3. Rowley JA, Sanders CS, Zahn BR, Badr MS. Gender differences in upper airway compliance during NREM sleep: role of neck circumference. J Appl Physiol. 2002. 92:2535–2541.4. Bijaoui EL, Champagne V, Baconnier PF, Kimoff RJ, Bates JH. Mechanical properties of the lung and upper airways in patients with sleep-disordered breathing. Am J Respir Crit Care Med. 2002. 165:1055–1061.5. Veldi M, Vasar V, Hion T, Vain A, Kull M. Myotonometry demonstrates changes of lingual musculature in obstructive sleep apnoea. Eur Arch Otorhinolaryngol. 2002. 259:108–112.6. Suratt PM, Dee P, Atkinson RL, Armstrong P, Wilhoit SC. Fluoroscopic and computed tomographic features of the pharyngeal airway in obstructive sleep apnea. Am Rev Respir Dis. 1983. 127:487–492.7. Veldi M, Vasar V, Hion T, Kull M, Vain A. Ageing, soft-palate tone and sleep-related breathing disorders. Clin Physiol. 2001. 21:358–364.8. Owen GO, Canter RJ, Robinson A. Snoring, apnoea and ENT symptoms in the paediatric community. Clin Otolaryngol. 1996. 21:130–134.9. Rosen CL. Clinical features of obstructive sleep apnea hypoventilation syndrome in otherwise healthy children. Pediatr Pulmonol. 1999. 27:403–409.10. Isono S, Shimada A, Utsugi M, Konno A, Nishino T. Comparison of static mechanical properties of the passive pharynx between normal children and children with sleep-disordered breathing. Am J Respir Crit Care Med. 1998. 157:1204–1212.11. Badr MS. Pathophysiology of upper airway obstruction during sleep. Clin Chest Med. 1998. 19:21–32.12. Strohl KP. Con: sleep apnea is not an anatomic disorder. Am J Respir Crit Care Med. 2003. 168:271–272. discussion 272-273.13. Schwab RJ. Pro: sleep apnea is an anatomic disorder. Am J Respir Crit Care Med. 2003. 168:270–271. discussion 273.14. Shepard JW Jr, Garrison M, Vas W. Upper airway distensibility and collapsibility in patients with obstructive sleep apnea. Chest. 1990. 98:84–91.15. Rivlin J, Hoffstein V, Kalbfleish J, McNicholas WT, Zamel N, Bryan AC. Upper airway morphology in patients with idiopathic obstructive sleep apnea. Am Rev Respir Dis. 1984. 129:355–360.16. Donnelly LF, Surdulescu V, Chini BA, Casper KA, Poe SA, Amin RS. Upper airway motion depicted at cine MR imaging performed during sleep: comparison between young patients with and those without obstructive sleep apnea. Radiology. 2003. 227:239–245.17. Gibson SE, Myer CM 3rd, Strife JL, O'Connor DM. Sleep fluoroscopy for localization of upper airway obstruction in children. Ann Otol Rhinol Laryngol. 1996. 105:678–683.18. Donnelly LF, Strife JL, Myer CM 3rd. Is sedation safe during dynamic sleep fluoroscopy of children with obstructive sleep apnea? AJR Am J Roentgenol. 2001. 177:1031–1034.19. Donnelly LF, Strife JL, Myer CM. Glossoptosis (posterior displacement of the tongue) during sleep: a frequent cause of sleep apnea in pediatric patients referred for dynamic sleep fluoroscopy. AJR Am J Roentgenol. 2000. 175:1557–1560.20. Suto Y, Matsuda E, Inoue Y, Suzuki T, Ohta Y. Sleep apnea syndrome: comparison of MR imaging of the oropharynx with physiologic indexes. Radiology. 1996. 201:393–398.21. Suto Y, Matsuo T, Kato T, Hori I, Inoue Y, Ogawa S, et al. Evaluation of the pharyngeal airway in patients with sleep apnea: value of ultrafast MR imaging. AJR Am J Roentgenol. 1993. 160:311–314.22. Uong EC, McDonough JM, Tayag-Kier CE, Zhao H, Haselgrove J, Mahboubi S, et al. Magnetic resonance imaging of the upper airway in children with Down syndrome. Am J Respir Crit Care Med. 2001. 163:731–736.23. Galvin JR, Rooholamini SA, Stanford W. Obstructive sleep apnea: diagnosis with ultrafast CT. Radiology. 1989. 171:775–778.24. Donnelly LF, Casper KA, Chen B. Correlation on cine MR imaging of size of adenoid and palatine tonsils with degree of upper airway motion in asymptomatic sedated children. AJR Am J Roentgenol. 2002. 179:503–508.25. Donnelly LF, Casper KA, Chen B, Koch BL. Defining normal upper airway motion in asymptomatic children during sleep by means of cine MR techniques. Radiology. 2002. 223:176–180.26. Abbott MB, Dardzinski BJ, Donnelly LF. Using volume segmentation of cine MR data to evaluate dynamic motion of the airway in pediatric patients. AJR Am J Roentgenol. 2003. 181:857–859.27. Donnelly LF. Obstructive sleep apnea in pediatric patients: Evaluation with cine MR Sleep studies. Radiology. 2005. 236:768–778.28. Leiter JC. Upper airway shape: Is it important in the pathogenesis of obstructive sleep apnea? Am J Respir Crit Care Med. 1996. 153:894–898.29. Shellock FG, Schatz CJ, Julien P, Steinberg F, Foo TK, Hopp ML, et al. Occlusion and narrowing of the pharyngeal airway in obstructive sleep apnea: evaluation by ultrafast spoiled GRASS MR imaging. AJR Am J Roentgenol. 1992. 158:1019–1024.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison between Echocardiography and Cardiac Cine-MRI : Left Ventricular Volume and Cardiac Output
- Comparison of Left and Right Ventricular Volume and Cardiac Output by MRI and Echocardiography
- Comparison of Nasotracheal Intubation and Tracheostomy in the Management of Upper Airway Obstruction in Children
- Comparison between Three-Dimensional Navigator-Gated Whole-Heart MRI and Two-Dimensional Cine MRI in Quantifying Ventricular Volumes
- A Case of Tracheostomy Induced Bilateral Tension Pneumothorax
