Acute Obstructive Cholangitis after Transarterial Chemoembolization: the Effect of Percutaneous Transhepatic Removal of Tumor Fragment
- Affiliations
-
- 1Department of Radiology, Eulji Medical Center, Eulji University College of Medicine, Seoul 139-711, Korea. ykchoman@eulji.ac.kr
- KMID: 1088733
- DOI: http://doi.org/10.3348/kjr.2009.10.2.197
Abstract
- Acute obstructive cholangitis due to the migration of necrotized tumor fragment is a rare complication occurring after a transarterial chemoembolization. The percutaneous tumor removal procedure following percutaneous transhepatic biliary drainage is an appropriate treatment over endoscopic removal for the relief of acute cholangitis in this case. Following this serial management, no invasive hepatocellular carcinoma of the bile duct recurred after two years of follow-up.
Keyword
MeSH Terms
-
Acute Disease
Bile Duct Neoplasms/pathology/therapy
Bile Ducts, Intrahepatic
Carcinoma, Hepatocellular/pathology/therapy
*Catheterization
Chemoembolization, Therapeutic/*adverse effects/methods
Cholangiography
Cholangitis/*etiology/therapy
Drainage
Humans
Jaundice, Obstructive/*etiology/therapy
Liver Neoplasms/pathology/therapy
Male
Middle Aged
Neoplasm Invasiveness
Neoplasm, Residual
Figure
-
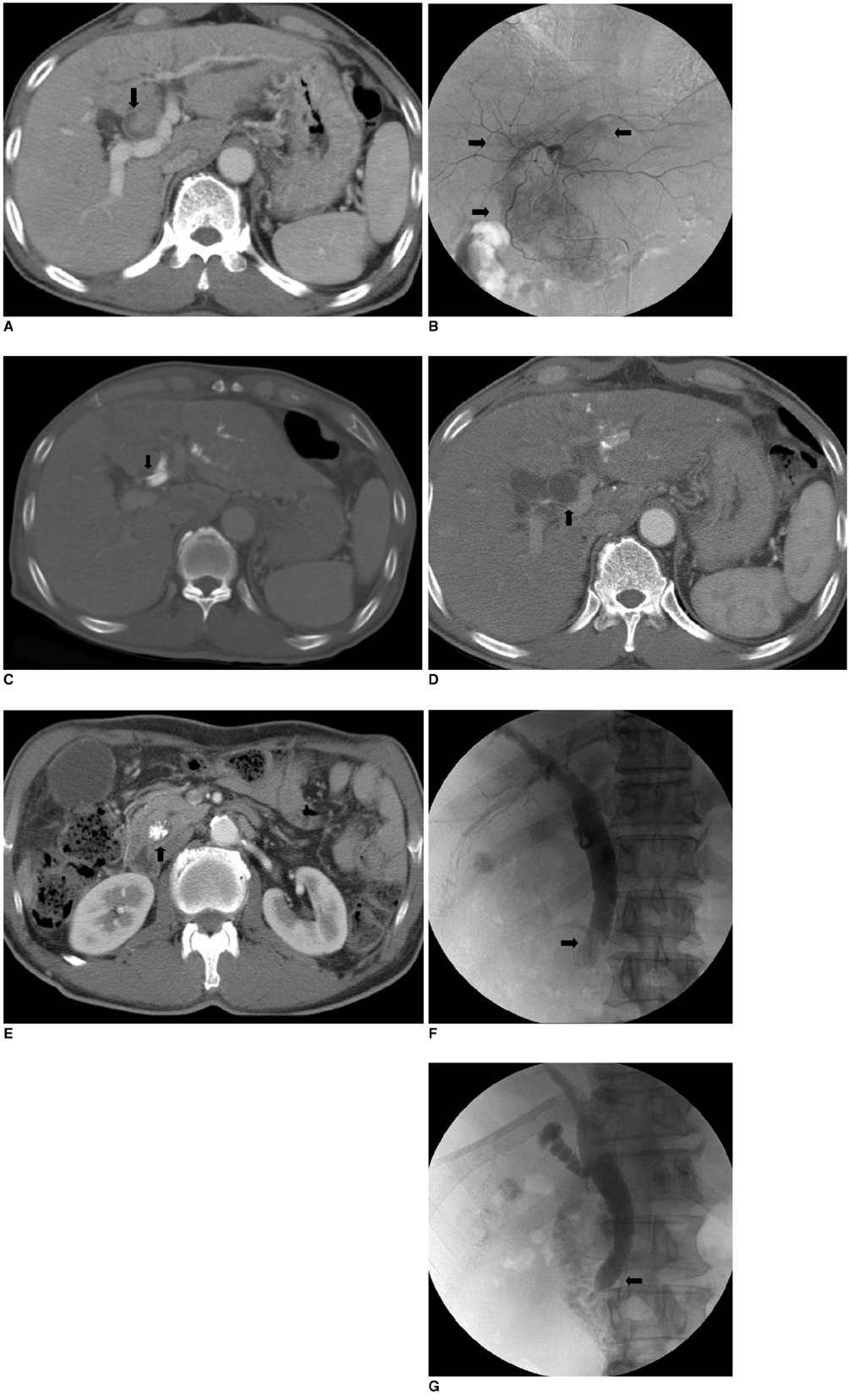
Fig. 1 Acute obstructive cholangitis after transarterial chemoembolization in 62-year-old male. A. Initial abdominal CT scan shows ovoid-shaped, highly enhancing invasive intraductal hepatocellular carcinoma in proximal common hepatic duct and left hepatic duct with ductal dilation (black arrow). B. Selective left hepatic angiography performed during initial transcatheter arterial chemoembolization showed ill-defined, tumor staining along proximal common hepatic duct and left hepatic duct (black arrows). Tumor staining occurred in identical location of bile duct invasion on CT image. C. Follow-up abdominal CT performed one week after initial transcatheter arterial chemoembolization showed multifocal, dense lipiodol deposits within proximal common hepatic duct and left hepatic duct after initial transcatheter arterial chemoembolization (black arrow). We also found small, faint, parenchymal lipiodol deposits in peripheral portion of left lobe. D. Follow-up abdominal CT performed two weeks after initial transcatheter arterial chemoembolization showed acutely dilated proximal common bile duct and left hepatic duct without visualization of previous lipiodol deposits at same level (black arrow). E. Same abdominal CT showed distally migrated, dense lipiodolized tumor fragments in distal common bile duct (black arrow), which was completely obstructed in distal common bile duct and resulted in dilatation of proximal common bile duct, left hepatic duct, and gallbladder. F. Percutaneous transhepatic biliary drainage was performed for treatment of obstructive jaundice. Cholangiography of percutaneous transbiliary drainage showed ovoid, large filling defect in distal common bile duct with complete obstruction of distal passage of contrast (black arrow). G. Final cholangiography performed after these procedures showed complete disappearance of tumor fragment in distal common bile duct, restoration of contrast passage into duodenum, and decompressed biliary tree (black arrow).
Cited by 2 articles
-
Acute Obstructive Cholangitis Complicated by Tumor Migration after Transarterial Chemoembolization: A Case Report and Literature Review
Hyung Chul Park, Hyun Bum Park, Cho Yun Chung, Min Woo Jung, Young Eun Joo, Sung Kyu Choi, Sung Bum Cho
Korean J Gastroenterol. 2014;63(3):171-175. doi: 10.4166/kjg.2014.63.3.171.Percutaneous Biliary Drainage Using Open Cell Stents for Malignant Biliary Hilar Obstruction
Sun Jun Ahn, Jae Ik Bae, Tae Sun Han, Je Hwan Won, Ji Dae Kim, Kyu-Sung Kwack, Jae Hee Lee, Young Chul Kim
Korean J Radiol. 2012;13(6):795-802. doi: 10.3348/kjr.2012.13.6.795.
Reference
-
1. Qin LX, Tang ZY. Hepatocellular carcinoma with obstructive jaundice: diagnosis, treatment and prognosis. World J Gastroenterol. 2003. 9:385–391.2. Hiraki T, Sakurai J, Gobara H, Kawamoto H, Mukai T, Hase S, et al. Sloughing of intraductal tumor thrombus of hepatocellular carcinoma after transcatheter chemoembolization causing obstructive jaundice and acute pancreatitis. J Vasc Interv Radiol. 2006. 17:583–585.3. Wang HJ, Kim JH, Kim JH, Kim WH, Kim MW. Hepatocellular carcinoma with tumor thrombi in the bile duct. Hepatogastroenterology. 1999. 46:2495–2499.4. Murata K, Shiraki K, Kawakita T, Yamamoto N, Okano H, Sakai T, et al. Hepatocellular carcinoma presenting with obstructive jaundice: a clinicopathological study of eight cases. Hepatogastroenterology. 2003. 50:2057–2060.5. Tantawi B, Cherqui D, Tran van Nhieu J, Kracht M, Fagniez PL. Surgery for biliary obstruction by tumour thrombus in primary liver cancer. Br J Surg. 1996. 83:1522–1525.6. Satoh S, Ikai I, Honda G, Okabe H, Takeyama O, Yamamoto Y, et al. Clinicopathologic evaluation of hepatocellular carcinoma with bile duct thrombi. Surgery. 2000. 128:779–783.7. Spahr L, Frossard JL, Felley C, Brundler MA, Majno PE, Hadengue A. Biliary migration of hepatocellular carcinoma fragment after transcatheter arterial chemoembolization therapy. Eur J Gastroenterol Hepatol. 2000. 12:243–244.8. Kobayashi S, Nakanuma Y, Terada T, Matsui O. Postmortem survey of bile duct necrosis and biloma in hepatocellular carcinoma after transcatheter arterial chemoembolization therapy: relevance to microvascular damages of peribiliary capillary plexus. Am J Gastroenterol. 1993. 88:1410–1415.9. Ando E, Tanaka M, Yamashita F, Kuromatsu R, Yutani S, Fukumori K, et al. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis: analysis of 48 cases. Cancer. 2002. 95:588–595.10. Hwang JY, Jang BK, Kwon KM, Chung WJ, Park KS, Cho KB, et al. Efficacy of hepatic arterial infusion therapy for advanced hepatocellular carcinoma using 5-fluorouracil, epirubicin and mitomycin-C. Korean J Gastroenterol. 2005. 45:118–124.11. Peng SY, Wang JW, Liu YB, Cai XJ, Deng GL, Xu B, et al. Surgical intervention for obstructive jaundice due to biliary tumor thrombus in hepatocellular carcinoma. World J Surg. 2004. 28:43–46.12. vanSonnenberg E, Ferrucci JT Jr. Bile duct obstruction in hepatocellular carcinoma (hepatoma)--clinical and cholangiographic characteristics. Report of 6 cases and review of the literature. Radiology. 1979. 130:7–13.13. Matsueda K, Yamamoto H, Umeoka F, Ueki T, Matsumura T, Tezen T, et al. Effectiveness of endoscopic biliary drainage for unresectable hepatocellular carcinoma associated with obstructive jaundice. J Gastroenterol. 2001. 36:173–180.14. Lee JW, Han JK, Kim TK, Choi BI, Park SH, Ko YH, et al. Obstructive jaundice in hepatocellular carcinoma: response after percutaneous transhepatic biliary drainage and prognostic factors. Cardiovasc Intervent Radiol. 2002. 25:176–179.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraductal migration of necrotic hepatocellular carcinoma: A possible cause of obstructive cholangitis after chemoembolization
- Acute Obstructive Cholangitis Complicated by Tumor Migration after Transarterial Chemoembolization: A Case Report and Literature Review
- Endoscopic Removal of Remained Drawstring After Percutaneous Transhepatic Biliary Drainage
- Percutaneous Transhepatic Transtumoral Biliary Drainage in a Patient with Obstructive Jaundice Due to Klatskin Tumor
- Percutaneous biliary drainage in acute suppurative cholangitis with biliary sepsis
